Enzyme-linked immunosorbent assay of phenolic glycolipid-I in patients with Hansen’s disease
Luis Hernando Moreno, MD1, Alberto Alzate, MD, MSP2
1. Professor and Director of Graduate Studies in Dermatology, Facultad de Salud, Universidad del Valle, Cali, Colombia.
e-mail: lhmorenom@hotmail.com
2. Professor of Epidemiology, Graduate Studies in Health, Universidad Santiago de Cali, Cali, Colombia.
e-mail: a_alzate@hotmail.com
Received for publication September 11, 2009 Accepted for publication February 23, 2010
SUMMARY
Introduction: Hansen’s disease or leprosy is a contagious-infection entity produced by the Hansen bacillus or Mycobacterium leprae. The phenolic glycolipid is a special trisaccharide found in the bacillus cell wall and proved to be specific and immunogenic species during M. leprae.
Objective: To determine the presence of the Hansen bacillus enzyme-linked immunoassay (ELISA) method glycolipid phenolic I in a group of patients in Dermatology Consultation at the Valle del Cauca Health Services; these patients were classified as cures or under watch according to criteria established by the World Health Organization (WHO).
Methodology: From the data base of the Dermatology Consultation at the Valle del Cauca Health Services, we studied 159 patients with Hansen’s disease who were tested with the enzyme-linked immunoassay (ELISA) with the phenolic glycolipid I to cross reference information and observe if they were or were not positive to this test. A positive ELISA indicates the bacillus is still present in the patient.
Results: As an important fact, we found that of 78 patients cured, when bearing in mind the monitoring period, 9 were positive for the ELISA. When this period was discarded, 81 sick individuals were classified as cured according to WHO criteria but the same 9 continued positive for ELISA.
Conclusion: It may be concluded that in spite of meeting WHO criteria, these patients still show presence of the bacillus and the monitoring period is not required as a criterion to discharge a patient. We recommend adding to WHO criteria a negative ELISA, to obtain additional information that helps to certify that a patient is or is not cured.
Keywords: ELISA; Hansen; Mycobacterium leprae; Phenolic glycolipid; Leprosy.
Inmunoensayo ligado a enzimas (ELISA) a glicolípido fenólico -1 en pacientes con enfermedad de Hansen
RESUMEN
Introducción: La enfermedad de Hansen o lepra es una entidad infecto-contagiosa producida por el bacilo de Hansen o Mycobacterium leprae. El glicolípido fenólico I es un trisacárido especial que se encuentra en la pared celular del bacilo y ha demostrado ser específico de especie e inmunogénico durante la infección de M. leprae.
Objetivo: Determinar la presencia del bacilo de Hansen por el método de inmunoensayo ligado a enzimas (ELISA) a glicolípido fenólico I en un grupo de pacientes del Consultorio Dermatológico del Servicio de Salud del Valle del Cauca clasificados como curados o en vigilancia, según criterios preestablecidos por la Organización Mundial de la Salud (OMS).
Metodología: De la base de datos del Consultorio Dermatológico del Servicio de Salud del Valle del Cauca se estudiaron en total 159 pacientes con enfermedad de Hansen a los cuales se les practicó examen de inmunoensayo ligado con enzimas (ELISA) con el glicolípido fenólico I a fin de cruzar información y observar si eran o no positivos a esta prueba. El ELISA positivo dice que el bacilo aún existe en el paciente.
Resultados: Se encontró como dato importante que de 78 pacientes curados, al tener en cuenta además el período de vigilancia, 9 fueron positivos para el ELISA. Cuando se descartó este período, a 81 enfermos se les clasificó como curados según criterios de la OMS pero siguieron positivos para ELISA los mismos 9.
Conclusión: Se concluye que a pesar de cumplir los criterios de la OMS, estos pacientes aún muestran presencia de bacilo y que el período de vigilancia no se necesita como criterio para dar de alta a un paciente. Se recomienda agregar a los criterios de la OMS el ELISA negativo, con el fin de tener una información más que ayude a certificar que un paciente está curado o no.
Palabras clave: ELISA; Hansen; Mycobacterium leprae; Glicolipido fenólico; Lepra.
Hansen’s disease or leprosy is a contagious infection pathology produced by an alcohol-acid resistant bacillus, known as Hansen’s bacillus or Mycobacterium leprae. M. leprae presents a triple coating rich in external polysaccharides and a basal peptidoglycan that forms the wall surrounding the cytoplasm. Peptidoglycans, arabinogalactans, and mycolates significantly contribute to the wall’s structural integrity, but do not contribute major immunogenicity to the bacteria. Other glycolipids, glycopeptidolipids, and trehalose containing lipooligosaccharides have been found to be active mycobacteria components. The most notable of the glycolipid molecules associated with the M. leprae cell wall is the phenolic glycolipid I (pgl-I), a special trisaccharide that has proven to be species specific and immunogenic during M. leprae infection1,2.
Clinically, this entity is characterized by the diversity in its presentation and its dependency on the conditions of the host, above all from the immunologic point of view. It is considered the main route of contamination of the upper respiratory pathway, although we cannot discard the role played in some instances by the sick skin. Currently, leprosy is considered an entity whose principal reservoir is the human being. The immunological conditions of the host are essential in determining any of the known clinical forms: undetermined, tuberculoid, dymorphous or borderline, and lepromatous. The undetermined form is a clinically and immunologically unstable condition of the disease. The tuberculoid form is a stable aspect of the disease; the smear is negative; the lepromin is positive. Lepromatous leprosy is another stable form of the disease, lepromin is negative, but there is presence of bacilli in the smears. It is a contagious form of the disease. The intermediate or borderline form is unstable and ends up in one in any of the tuberculoid or lepromatous stable forms. Mycobacteria are present, although not in the proportion as in the lepromatous form; the Mitsuda reaction is generally slightly positive. It is another contagious form of the disease3.
Analysis of the circulating immune complex in patients, above all those with phenolic glycolipid I as a specific antigen and the role of macrophages has gained importance in diverse research works and has led to better understanding this disease3-10. Furthermore, a correlation has been noted between the bacillary index and the presence of the phenolic glycolipid I antigen in serum of patients and it has been shown that levels of antibodies towards this antigen diminish when treatment starts11.
For the diagnosis of the disease and follow up of patients, different laboratory methods are employed like the smear, the biopsy, and the lepromin. A clinical exam and a good clinical history are vitally important. However, it is difficult to precisely define if a patient is or is not cured, and if the bacillus persists in the patient’s organism with the previous laboratory methods.
The enzyme-linked immune-absorbent assay (ELISA) is a method that has acquired scientific credibility and it is currently used to diagnose diverse diseases like tuberculosis, dengue, rubella, and HIV, among others. Brennan and Hunter9 managed to characterize phenolic glycolipid I as a specific M. leprae antigen. Seroepidemiologic studies in different countries to diagnose the infection, have permitted evaluating the ELISA test with a special antigen, phenolic glycolipid I; works have been done with serum from both paucibacillary and multibacillary patients, in whom sensitivity has been between 82 and 100% for the multibacillary and between 5 and 54.5% for the paucibacillary with a global sensitivity between 43.8% and 62.8%. Specificity in endemic and non-endemic areas varied between 82% and 100%3.
With ELISA-type tests at antibody level in different populations, it has been shown that:
The serologic response to this antigen from individuals infected is of IgM type12,13. The level of antibodies corresponds to the bacilli load and increases, then, from the tuberculoid pole to the lepromatous12,14. Almost all patients with the lepromatous form have antibodies for this antigen14. Antibody levels diminish with chemeotherapy15. Seropositivity seems to precede the clinical manifestations of lepromatous patients15. In studies with household contacts of leprosy patients, it has been found that 30% offer a positive response to these types of tests, but most do not develop the disease16-18.
The Hansen ELISA is an indirect immune-enzymatic test. It is worth noting that the titles are positive when the antigen is present and we are dealing with a case of leprosy; they are negative when there is no presence of antigen and it may be excluded as a case. It has been recommended that in the screening results the following values should be used according to the ratio of the fluorescence of the serum researched with respect to the positive control serum: less than 0.3, negative; 0.3-0.4, doubtful; 0.4-0.5, suspect; and greater than 0.5, elevated19,20.
Through the current study, we sought to find the correlation between the behavior of Hansen’s disease in its different clinical states and its evolution with respect to the ELISA method. We also compared this method to those used traditionally to monitor patients such as the smear and, above all, the clinical evaluation.
METHODS
Herein, we studied 159 patients with confirmed diagnosis of Hansen’s disease. Respective and previously defined samples were taken from the patients. Included in the study were patients who were registered as sick within the last three years, in addition to those who were in the surveillance period and those who has been discharged as cured. Three groups were formed; the first group gathered those patients who were under control within the last three years; the second group included patients in the surveillance period, and the third group took in those patients who had left the program as cured. The study also included 20 patients with non-lepromatous tuberculosis for the purpose of evaluating the behavior of the Hansen ELISA technique against the Koch bacillus as a microorganism different from M. leprae and that could eventually have a crossed reaction in this test.
The project was approved by the Ethics Committee of the Faculty of Health at Universidad del Valle, Cali, Colombia, and each patient signed an informed consent prior to taking the blood sample. For the ELISA tests, we used the UMELISA HANSEN equipment that detects M. leprae IgM antibodies via fluorescence.
The data were recorded in an Excel data base and they were analyzed by using the Epi Info program version 6.0 to find the average, mode, and median for each variable according to whether it is categorical or continuous, estimate its standard error and deviation for averages or proportions and, thus, calculate the reliability intervals from each of the variables.
The risk factors to become ELISA positive were analyzed on a four-cell table, where the dependent variable is to continue positive for the phenolic glycolipid I antigen after being considered cured according criteria currently employed like: time of treatment for each clinical form, negative smear, remission of symptoms and medical signs, and regularity of treatment; also analyzed was the surveillance time used.
The currently accepted cure criteria are:
Disappearance of clinical lesions. Negative smear. Adequate treatment scheme according to clinical form. Regularity during treatment.
Stemming from this definition of cure, we calculated sensitivity. Since it is expected that the ELISA test become the definite cure evidence, sensitivity and specificity were analyzed, as well as the positive and negative predictive values of the criteria used in this study and the statistical significance was estimated in agreement between both criteria (ELISA and «cure») through Cohen’s Kappa test.
RESULTS
We studied 159 patients with Hansen’s disease (leprosy); 81 were under treatment and 78 were cured according to clinical cure criteria, negative smear, and adequate pharmacological treatment scheme for each form of the disease. The surveillance period previously used was also considered as additional criteria to discharge patients and evaluate if it is recommended to continue with the surveillance. Of the total number of patients, 130 corresponded to the multibacillary form (66 cured and 64 under treatment) and 29 to the paucibacillary form (11 cured and 18 under treatment). The 20 patients with tuberculosis were ELISA negative, as expected (Table 1).
Of the 159 patients, 12 corresponded to dymorphous leprosy (DL), 9 to undetermined (UL), 118 to lepromatous (LL), and 20 to tuberculoid (TL); that is, 130 multibacillary (MB) and 29 paucibacillary (PB). Patient ages ranged from 5 to 93 years of age (Table 2).
Of the 26 patients with elevated ELISA, 25 are LL and 1 LD. With suspect ELISA of the total of 27, 23 are LL, 1 LD, 2 LT, and 1 LI. Of the 106 with normal ELISA, 70 are LL, 10 LD, 18 LT, and 8 LI. The differences do not manage to be statistically significant (p=0.05814026) because of the cells with very small values or equal to zero.
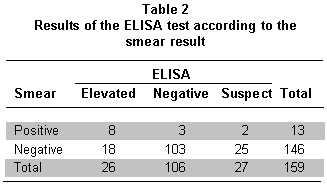
Of the 26 patients with elevated ELISA, 18 show negative smear and 8 are positive. With suspect ELISA in 27 patients, 2 are positive and 25 negative. With a normal ELISA test in 106 patients, 3 are positive for the smear and 103 are negative. The statistical value is p=0.00001724, significant statistical difference. It was expected for the negative smears to also be negative ELISA under 0.3 according to standard figures given by previous studies (Table 3).
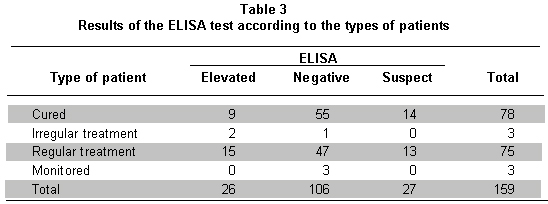
Of the 78 patients considered cured, 9 had elevated ELISA and 14 had suspect ELISA. Only 55 of the 78 were negative. Of the patients with regular treatment, 28 had elevated or suspect ELISA and 47 had already become negative through treatment.
DISCUSSION
Hansen’s disease (leprosy) continues to be a public health problem in the world. Throughout the history of humanity, many efforts have been made to better understand this entity and reach its elimination and subsequent eradication. This disease bears a historic load that makes it feared by everyone. All scientific research undertaken to understand it and treat it in the best possible way are valid and should be considered. This entity reveals immunological behavior that is special and fascinating for any researcher. Since 1943, when diaminodiphenylsulfone (DDS) therapy was introduced, and passing through the establishment of multidrug therapy, the world’s medical and scientific community has dreamt of eradicating this condition. Criteria have been unified to define if a patient is cured or not of the disease and what’s more, in many instances it is difficult conduct an asserted diagnosis. It is common to find relapses in individuals thought to be cured. For this purpose, surveillance was instituted – initially for a lifetime. Then, this surveillance time was reduced to two years for paucibacillary patients and five years for multibacillary patients; all this in agreement with diverse clinical-epidemiological and bacteriological studies that have been carried out. Currently, the conduct recommended by the World Health Organization (WHO) and the Colombian Ministry of Health is to consider as cured every patient WHO:
Receives adequate stipulated time of treatment for diverse clinical forms. Is clinically cured. Has a negative smear; i.e., the patient is no longer under surveillance.
However, there is no absolute certainty as to when a patient is free from the bacillus. Clinical improvement, time of treatment, adequate chemotherapy, and negative smear are the methods currently employed to discharge patients suffering or who suffered this disease. There must be sufficient clear motives to discharge a leprosy patient and consider such cured and avoid relapse as much as possible. Because phenolic glycolipid-I is characteristic of the M. leprae, it has permitted defining the presence of the bacillus in organisms of patients or possible patients. This definition is accomplished through indirect techniques like the enzyme-linked immuno-absorbent assay (ELISA) test.
In the current study, we found no statistical difference in age or gender of patients and the greatest number of these corresponded to multibacillary forms, i.e., those considered contagious, which endorses every action and/or recommendation for proper treatment of this entity. We consider it important to suggest the execution of the compared surveillance period, again as a cure criterion, given that it is another motive that when added to the ELISA results would furnish tools to aid in deciding if a patient is free from the disease or does not support the disease.
The most important aspect was to find patients who considered themselves cured with high levels of ELISA, suggesting that these were cases of sub-clinical patients that should be watched closely or, ideally, receive treatment until the test proves negative. ELISA is proposed as an additional criterion, which if added to those currently used would yield greater certainty on the cure of the patient with Hansen’s disease and would bring us closer to whether or not the patient is free from the bacillus. Greater numbers of cure criteria available will improve the patient’s welfare and that of the community in general. Furthermore, we propose that the values to define whether a title is high, suspect, doubtful, or negative should be adjusted and we suggest that only values lower than 0.40 be used for negative titles and those greater than 0.40 for positive titles, which would further simplify the analysis that added to pre-existing criteria lead to precise conclusions and actions according to the values obtained.
Furthermore, we suggest that individuals in contact and those living with the patients -especially multibacillary patients- undergo an ELISA test as part of its surveillance to discover possible early or sub-clinical cases of the disease and follow proper conduct. It is important to highlight that a patient can remain positive for the disease through multiple causes like irregularity in its treatment, inadequate time of treatment, and lack of clear criteria to establish if the patient is indeed cured and can be discharged. Additionally, it is obligatory to manifest the importance of the population follow up (contacts and cohabitants) and the use of lepromin, which along with the ELISA test would help in deciding if an individual should or should not receive treatment or should be merely observed with clinical and/or laboratory follow up.
This research presents the following list of conclusions:There is no precise method that tells exactly when a leprosy patient is cured from the disease. To discharge a leprosy patient, there must be abundant clinical motives and laboratory aids. ELISA is a laboratory test that helps to determine if a patient is free or not from the Hansen bacillus. It is necessary to conduct surveillance again in the follow up of patients with Hansen’s disease who complete the treatment cycles. According to the results from the current research, ELISA is recommended as a laboratory test for patients with leprosy who are going to be discharged and who meet currently accepted requirements: clinical cure, adequate treatment, compliance with time of treatment, surveillance, and negative smear.
Conflict of interest. None of the authors has conflicts of interest related to this study.
REFERENCES
1. Britton WJ, Lockwood DN. Leprosy. Lancet. 2004; 363: 1209-19.
2. Casal M, Linares MJM. Tuberculosis, M. leprae y micobacteria atípicas. En: Microbiología médica general. Madrid: Editorial Mosby; 1996. p. 378.
3. Rodríguez G, Orozco LC. Lepra. Bogotá, DC: Instituto Nacional de Salud; 1996.
4. Abe M, Ozawa T, Minagawa F, Yoshino Y. Estudios inmunoepidemiológicos sobre la infección subclínica en lepra. Rev Front Leprol. 1993; 299-300.
5. Lal H, Jain VK, Mittal RA, Chaudhary SD, Saini V. Detección de anticuerpos frente al glicolípido fenólico por ELISA en pacientes de lepra. Vol Indian J Lepr. 1993; 65: 95-9.
6. Bagshawe AF, Roger JG, Karl B, Lyn A. IgM serum antibodies to phenolic glycolic and clinical leprosy. Intern J Leprosy Mycobact Dis. 1990; 58: 25-307.
7. Montoya D, Cruz D, Teles RM, Lee DJ, Ochoa MT, Krutzik SR et al. Divergence of macrophage phagocytic and antimicrobial programs in leprosy. Cell Host Microbe. 2009; 6: 343-53.
8. Cho SN, Cellona RV, Fajardo TT Jr, Abalos RM, de la Cruz EC, Walsh GP et al. Detection of patients treated with various drug regimens. Intern J Leprosy Mycobact Dis. 1991; 59: 25-31.
9. Hunter SW, Brennan PJ. A novel phenolic glycolipid from Mycobacterium leprae possibly involved in immunogenicity and pathogenicity. J Bacteriol. 1981; 147: 728.
10. Brett SJ, Payne SN, Gigg J, Buergess P, Gigg R. Use of synthetic and inmunodominant epitope of phenolic glycolipid in the serology of leprosy. Clin Exp Inmunol. 1986; 64: 476-83.
11. Cho SN, Cellona RV, Villahermosa LG, Fajardo TTJr, Balagon MV, Abalos RM et al. Detection of phenolic glycolipid I leprae in sera from leprosy patient start of multidrug therapy. Clin Diagn Lab Inmunol. 2001; 8: 138-42.
12. Hussain R, Jamil S, Kifayet A, Firdausi F, Dockrell HM, Lucas S et al. Quantitation of IgM antibodies to the M. leprae synthetic disaccharide can predict early bacterial multiplication in leprosy. Intern J Leprosy Mycobact Dis. 1990; 58: 491-501.
13. Lefford MJ, Hunegnaw M, Siwik E. The value of IgM antibodies to PGL- in the diagnosis of leprosy. Intern J Leprosy Mycobact Dis. 1991; 59: 432- 40.
14. Shripad AP. Screening of anti-M. leprae antibodies in the blood samples eluted from filter paper blood blots. Intern J Leprosy Mycobact Dis. 1990; 58: 123-6.
15. Batch MA, Wallach D, Flageul B, Hoffenbach A, Cotteno TF. Antibodies to phenolic-glycolipid I and Mycobacterium leprae in leprosy patients: evolutions during therapy. Intern J Leprosy Mycobact Dis. 1986; 54: 256-67.
16. Meeker HC, Schuller GL, Fusco F, Giardina-Becket MA, Sersen E, Levis WR. Sequential monitoring of leprosy patients with serum antibody levels to phenolic glycolipid I, a synthetic analog of phenolic glycolipid I and mycobacterial lipoarabinomanan. Intern J Leprosy Mycobact Dis. 1990; 58: 503-11.
17. Laferte J, Abreu EG, Robaina R, Pérez V. UltramicroELISA para detección de IgM anti M. leprae. Rev Inst Med Trop São Paulo. 1991; 33: 491-5.
18. Mora N. Determinación de anticuerpos anti-glicolípido fenólico-I en población general de un área endémica de lepra. Rev Leprol FONTILES. 1992; 18: 587-97.
19. Tomella A, Solís RI, Pérez I, Medina Y, Kerguele C, Olaya P. UMELISA-Hansen en el diagnóstico y seguimiento de la lepra. La Habana: Centro de Inmunoensayo; 1992.
20.González OCE, Abreu A. Vigilancia de la lepra en situaciones de baja prevalencia. Rev Panan Salud Publ. 2001; 9: 97-8.