Quality of life in persons living with HIV–AIDS in three healthcare institutions of Cali, Colombia
Claudia Patricia Valencia, MSc1, Gladys Eugenia Canaval, PhD1, Diana Marín2, Carmen J. Portillo, PhD3
1. Professor, Research
Group on Health Promotion ( PROMESA), School of Nursing, Universidad
del Valle. Cali, Colombia. Member of the International Nursing and HIV
-AIDS Research Network.
e-mail: claudia.p.valencia@correounivalle.edu.co glacanav@univalle.edu.co
2. Statistician, Hospital Epidemiology, Hospital Universitario del Valle, Cali, Colombia. e-mail: dmarin@hotmail.com
3. Professor School of
Nursing, University of California, Co-Director International Nursing
and HIV -AIDS Research Network. e-mail: cportillo@nursing.ucsf.edu
Received for publication November 4, 2008 Accepted for publication March 18, 2010
SUMMARY
Antecedents: The
Human Immunodeficiency Virus is currently considered a chronic disease;
hence, quality of life is an important goal for those suffering the
disease or living with someone afflicted by the virus.
Objectives:
We sought to measure the quality of life in individuals living with
acquired immunodeficiency syndrome virus and establish its relationship
with socio-demographic and clinical variables.
Methods:
This is a cross-sectional, descriptive study with a sample of 137
HIV-infected individuals attending three healthcare institutions in the
city of Cali, Colombia. Quality of life was measured via the
HIV/AIDS-Targeted Quality of Life (HAT-QoL) instrument. The descriptive
analyses included mean and standard deviation calculations. To
determine the candidate variables, we used the student t test and the
Pearson correlation. The response variable in the multiple linear
regression was the score for quality of life.
Results:
Some 27% of the sample were women and 3% were transgender; the mean age
of the sample was 35 + 10.2 years; 88% had some type of health
insurance; 27% had been diagnosed with AIDS, and 64% were taking
antiretroviral medications at the time of the study. Quality of life
was measured through a standard scale with scores from 0 to 100.
Participants’ global quality of life mean was 59 + 17.8. The
quality-of-life dimensions with the highest scores were sexual
function, satisfaction with the healthcare provider, and satisfaction
with life. The highest quality-of-life scores were obtained by
participants who received antiretroviral therapy, had health insurance,
lower symptoms of depression, low frequency and intensity of symptoms,
and no prior reports of sexual abuse. Eight variables explained 53% of
the variability of the global quality of life.
Conclusions: Those receiving antiretroviral therapy and who report fewer symptoms best perceived their quality of life.
Implications for
practice: Healthcare providers, especially nursing professional face a
challenge in caring to alleviate symptoms and contribute to improving
the quality of life of their patients.
Keywords: Quality of life; Symptoms,; HIV; AIDS; Health; Care; Nursing.
Calidad de vida en personas con VIH-SIDA en tres instituciones de salud de Cali, Colombia
RESUMEN
Antecedente:
Hoy en día se considera el VIH como una enfermedad
crónica; por tanto,la calidad de vida es una meta importante de
alcanzar en las personas que viven y conviven con el virus.
Objetivos:
Medir la calidad de vida en personas que viven con el virus del sida y
establecer la relación con variables socio-demográficas y
clínicas.
Métodos:
Estudio transversal, descriptivo, con muestra no probabilística
de 137 personas con VIH que asistieron a tres instituciones de salud de
Cali, Colombia. La calidad de vida se midió con el instrumento
Hiv/Aids-Targeted Quality of Life (HAT-QoL). El análisis
descriptivo incluyó los cálculos de promedio y
desviación estándar. Para determinar las variables
candidatas se utilizaron la prueba t de Student y la correlación
de Pearson. La variable respuesta en la regresión lineal
múltiple fue el puntaje de calidad de vida.
Resultados:
De los encuestados 27% eran mujeres y 3% transgéneros; la edad
promedio fue 35 + 10.2 años; 88% tenían algún tipo
de seguro de salud; 27% con diagnóstico de Sida y 64% con
tratamiento antirretroviral en el momento del estudio. La calidad de
vida se midió con una escala estandarizada de 0 a 100; el
promedio de calidad de vida global fue de 59 + 17.8; las dimensiones de
calidad de vida que mayor puntaje obtuvieron fueron la función
sexual, la satisfacción con el proveedor de cuidados de salud y
la satisfacción con la vida. Los puntajes más altos en
calidad de vida los obtuvieron personas que recibieron tratamiento
antirretroviral, con acceso a algún seguro de salud, menor
sintomatología depresiva, baja frecuencia e intensidad de
síntomas y sin antecedentes de abuso sexual. Ocho variables
explicaron 53% de la variabilidad de la calidad de vida.
Conclusión:
Las personas que reciben tratamiento antirretroviral y que informan
menos síntomas son quienes mejor perciben su calidad de vida.
Implicaciones para la práctica. Los proveedores de salud
especialmente los profesionales de enfermería tienen un reto en
el cuidado para aliviar los síntomas y hacer un aporte a la
calidad de vida de los pacientes.
Palabras clave: Calidad de vida; Síntomas; VIH; Sida; Salud; Cuidado; Enfermería.
Herein, we introduce
the results obtained on quality of life from the third study titled
«Symptoms and self-care in people with HIV-AIDS»1-3
conducted in different nodes by the International Nursing and HIV-AIDS
Research Network, led by the University of California. This article
presents the results from the node in the city of Cali, Colombia.
The
concept of health and its relationship with quality of life has been
suggested by several authors from different approaches. Health has been
traditionally seen as an aspect opposed to disease, even though the
World Health Organization (WHO) redefined it over five decades ago as a
state of complete wellbeing, still today health and its promotion are
not emphasized by the programs of healthcare providers for individuals
with some diagnosis of chronic disease like that related to Human
Immunodeficiency Virus-Infected Individuals (PLWHA); this has led
healthcare providers and researchers to make measurements of the health
and wellbeing of individuals in very limited manner4.
Quality
of life is a goal of health systems and of public health policies;
quality of life is currently a measurement that indicates the lack of
or presence of wellbeing, it is a measurement that is used as a
positive indicator regarding individuals’ relationship with
health and it is used to measure the effects or its relationship with
disease4.
Quality
of life is a term implying happiness and satisfaction with life and
adequate functioning. It is a very broad term and conceptually quite
complex; furthermore, it is a multidimensional concept. Health is one
of the dimensions of quality of life, but it is not the only one; other
dimensions have to do with financial aspects, interrelationships,
sexuality, work, as well as cultural and spiritual aspects5.
The path of the HIV disease is characterized by episodes of acute exacerbation and long periods of relative health6.
If the HIV disease advances, the result is diminished quality of life.
Although quality of life is a multidimensional construction that does
not accomplish universal agreement, some agreements have been reached
regarding its relationship with7. The WHO defines it as the
individual perception of the position towards life within the context
of culture and value systems in which individuals live in relation to
their goals, expectations, standards, and concerns4.
Quality
of life is a particularly important measurement to determine the
effects of the HIV-AIDS disease. Bearing in mind that this is a chronic
disease and that the life expectancy of Human Immunodeficiency
Virus-Infected Individuals (PLWHA) is increasing because of
developments in treatments and the dramatic change in mortality
measurements, we do not expect deaths of individuals infected by this
virus if treatment is appropiate8. In spite of this, it has
been reported that antiretroviral therapy (ARV) causes symptoms that
affect, to a greater or lesser degree, PLWHA and impacts on their
quality of life9.
Objectives
1. To measure the quality of life in a sample of individuals living with the AIDS virus in the city of Cali, Colombia.
2. To identify the
relationship between global quality of life and its specific dimensions
to some clinical and socio-demographic variables.
METHODOLOGY
Cross-section,
observational, and descriptive study conducted between 2005 and 2006,
with a non random sample of 137 patients with HIV-AIDS attending
ambulatory services at three healthcare institutions in Cali. The
patients were approached on the day of their medical or nursing
consultation and those who accepted voluntary participation and had the
availability of time to answer the survey were included. Among the
inclusion criteria defined were: subjects over 18 years of age, with or
without antiretroviral therapy, and with or without AIDS diagnosis at
the time of the study.
The
instruments used in measuring the variables included in the study have
been broadly validated in different research projects and are of free
distribution and use; these are: Demographic data questionnaire (age,
gender, social security), Depression Scale from the Center for
Epidemiological Studies [Escala de Depresión del Centro de
Estudios Epidemiológicos (CES-D)], Revised Signs and Symptoms
Checklist in people with HIV (SSC-HIVrev), HIV/AIDS-Targeted Quality of
Life (HAT-QoL) instrument.
Depression Scale from the Center for Epidemiological Studies (CES-D). Measures
symptoms of depression; it has 20 statements, responses range from 0
(never or rarely) to 3 (almost always or always). The total sum may
range from 0 to 60 and a score of 16 or more indicates the need for a
diagnostic evaluation for major depression. An estimated Alpha
coefficient of 0.90 was obtained in a sample of 727 AIDS patients9.
Revised Signs and Symptoms Checklist in people with HIV (SSC-HIVrev).
This is a 3-part checklist. Part I consists of 45 points and 11
factors, with confidence estimates ranging from 0.76 to 0.91; Part II
consists of 19 symptoms related to HIV/AIDS, which are not grouped into
factors but which can be of interest from the clinical perspective; and
Part III has eight points related to gynecological symptoms. These
eight points were subjected to principal components factor analysis
with varimax rotation (N = 118 HIV positive women), which yielded a
solution of a factor that explained 71.8% of the variability; the
confidence measurement of 0.9410.
HIV/AIDS-Targeted Quality of Life (HAT-QoL). This is a specific instrument to measure quality of life in Human Immunodeficiency Virus-Infected Individuals (PLWHA)11.
It has nine dimensions: «General Function» (which is a
combination of the physical and social functions); «satisfaction
with life»; «concerns about health»; «financial
concerns»; «concerns about medications»;
«concerns about their HIV condition»; «concerns about
disclosing their diagnosis»; «confidence in the healthcare
provider»; «sexual function». The total final
evaluation was transformed into a linear scale from 0 to 100, where 0
is the worst possible score and 100 is the best possible score.
The Project was
approved by the Human Ethics Review Institutional Committee at
Universidad del Valle. Prior to applying the data gathering instrument,
the informed consent form was read explaining the objectives of the
study and the conditions of free and voluntary participation. All the
participants signed the informed consent form.
Data analysis. For
the descriptive analysis of quantitative variables like quality of life
and frequency of symptoms, the mean and standard deviation were
calculated and percentages were calculated in categorical variables.
The bivariate analysis to determine differences in quality-of-life
scores included the verification of the normality assumption with the
Kolmogorov-Smirnov (K-S) test, the Student t test, and calculation of
the Pearson correlation. The 95% confidence interval (CI95%) was
calculated for measurement differences. The linear regression was used
to determine the factors related with quality-of-life scores. The
purpose with the construction of this model was more explicative than
predictive, which is why no variable selection method was used. The
global adjustment of the model was verified with the one-way ANOVA; the
pertinence of each variable was verified via the statistical t test;
fitting of the model was verified with the adjusted determination
coefficient and the assumptions of residues were verified through the
following manner:
1. Normality and zero means: with the K-S test, the Q-Q plot, and the residue histogram
2. Homoscedasticity: via residue plot versus predicted values.
3. No self-correlation: with the Durbin-Watson statistical package.
4. Multicollinearity: with the Variance Inflation Factor (VIF)
The results were analyzed via the SPSS version 13 statistical package.
RESULTS
The results were
handled per instructions by the authors. The population studied
consisted of 96 (71%) men, 37 (27%) women, and 4 (3%) transgender; 88%
of the subjects reported having some type of health insurance, most
(57.3%) belonged to the subsidized healthcare regime of the Health and
Social Security System. Twenty-seven percent had been diagnosed with
AIDS and 64% were receiving antiretroviral therapy at the time of the
study. Regarding age, the mean was 35.3 + 10.2 years with a range from
20-73 years, 9% were above 50 years of age. The day of the interview,
the participants reported an average of 17+11 symptoms, the data of the
characteristics of the sample are published in depth in another article
by Valencia et al.1
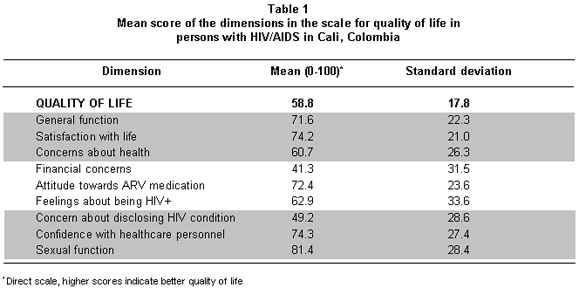
Quality of life. The average global quality-of-life score in the sample of patients was 59+17.8 points in a standardized scale from 0-100. Table 1
shows the score for each of the nine quality-of-life dimensions. Note
that the lowest scores in the dimensions correspond to financial
concerns (41.3) and to the difficulty of disclosing their HIV condition
(49.2). The dimensions revealing the best scores are sexual function
(81.4), satisfaction with life (74.2), and satisfaction with attention
received from healthcare personnel (74.3).
The
bivariate analysis per healthcare regime (type of insurance) revealed
that individuals in the contributive regime had a better global score
on the quality-of-life scale compared to the global score of
individuals with subsidized regime (average: 66.21 vs. 53.8,
respectively; p=0.00). These statistically significant differences are
also observed in the scores for the following dimensions:
«general function», «concerns about health»,
«financial concerns», and «concerns about their HIV
condition» (Table 2). Regarding sex,
statistically significant differences were only found in the dimension
on concerns about health, which is lowest for the female group (52.8
vs. 63.5; p=0.032).
Upon
analyzing quality of life according to age, statistically significant
difference was only found in the dimension for «confidence with
the attention offered by the healthcare provider»; this being the
highest quality-of-life score for those over 50 years of age (93 vs.
72.4; p=0.0120).
No
statistically significant differences were observed between individuals
with or without children under their care. Regarding the relationship
between quality of life and treatment or not with antiretroviral
medication therapy (ARV), it was found that quality of life is
generally better for those taking the medications than for those who
were not taking them (66 vs. 46; p=0.00). Analyzing the relationship
between ARVT and the different dimensions of the scale, significant
differences were noted in the dimensions dealing with «financial
concerns and concerns about disclosing their HIV+ condition»
(47.6 vs. 30; p=0.001 and 70.1 vs. 49.7; p=0.000, respectively). To
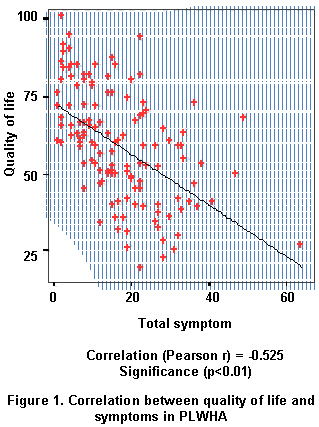
explore the relationship between symptoms and quality of life, we
measured the relationship with the average frequency of symptoms, the
intensity of the symptoms, and the symptoms of depression. The score
for quality of life was lower among those with symptoms of depression
– both in the global score (63.9 vs. 51.97; p=0.000) and in the
dimensions of general function (p=0.000), concerns about health
(p=0.02), concerns about their HIV condition, concerns about ARV
medications (p=0.008), and sexual function (p: 0.005). The Pearson
correlation between quality of life and frequency of symptoms revealed
that as symptoms increase the quality of life is impaired (r: -0.525
p<0.05) (Figure 1).
Multivariate analysis. To
determine factors related to quality of life and its nine dimensions,
we used a multiple linear regression for global quality of life and
nine models separated for each of the dimensions. Eight of the nine
variables included in the model for quality of life explain 53% of the
variability in quality-of-life scores; however, it was found that only
the frequency of symptoms and the use of ARV therapy are significant to
explain quality of life (p<0.01). The negative coefficient (-.340,
t=-4.962, p=0.000), for the first variable, indicates that the number
of symptoms increase in an individual with HIV, global quality of life
diminishes; the positive coefficient (.437, t=6.335, p=0.000), for the
second variable, indicates that individuals who received ARV therapy
have better quality of life than those who did not receive it. The
model fulfills all the statistical suppositions; no multicollinearity
problems were found, and the variance was homoscedastic and the
distribution of residues was normal.
Table 3
shows the regression models for the dimensions with the greatest number
of independent variables. It is noted that the amount of symptoms
(frequency of symptoms) negatively affects the following dimensions:
general function, satisfaction with life, concerns about health, and
concerns about medications. For the dimension on concern about being
HIV+, the bivariate or multivariate analyses did not reveal variables
to explain that dimension.
Increased
frequency of symptoms, the presence of depression, sexual abuse, and
being over 50 years of age negatively affect the dimension of
«satisfaction with life». These variables explain 31.8% of
the variance for this dimension. In the dimension on concern about ARV
medications, it is noted that taking them improves the quality of life
in said dimension by 26%, and along with the physical abuse and
frequency of symptoms variables help to explain 45% of the variability
in that dimension.
Individuals
over 50 years of age (p=0.021) who are in the contributive healthcare
regime (p=0.003), have greater scores in the dimension of
«confidence with the healthcare provider»; both variables
-along with the constant- explain 21.1% of the global variability of
that dimension. In other dimensions, it is noted that quality of life
is affected by symptoms of depression and by being or not being
affiliated to healthcare insurance; the dimension on «financial
concerns» is negatively affected in individuals with
subsidized-type healthcare regime; the sexual function dimension is
most affected in individuals suffering from depression (p=0.016).
DISCUSSION
The results in this
study agree with reports from other studies; diverse factors like the
symptoms perceived by PLWHA have been associated to lower
quality-of-life scores12; likewise, some social characteristics have been associated with a low quality-of-life index13.
In contrast, factors like middle or high economic level in terms of
income and not having children under their care have been associated to
better quality of life14. In general terms, it is observed
that the global variability explained by the variables in each of the
dimensions is quite high compared to results obtained by Phaladze et
al.7
In this
study, the patients with the highest quality-of-life scores had better
access to healthcare services. Those affiliated to a contributive
healthcare regime had better-quality services; presenting fewer
financial concerns, fewer symptoms of depression, received
antiretroviral therapy, and experienced lower frequencies and
intensities of symptoms; they also evidenced fewer antecedents of
sexual or physical abuse. These findings are similar to those reported
by Phaladze et al.7 who found a close correlation between
intensity of symptoms and low quality of life, at the expense of
patients’ functional capacity impairment. Our results, like
others, show that high frequency and intensity of symptoms have
negative effects on quality of life15,16 and on satisfaction for life; additionally, increased states of depression impairs quality of life.
Several studies13,17,18
have identified an inversely proportional relationship between quality
of life and poverty, as suggested by the results in this study. Hence,
the socioeconomic conditions determine greater vulnerability in
acquiring the infection, as well as in living with a better quality of
life. This phenomenon denotes the continuity of the chain of social
factors characterizing this disease, turning it into a vicious circle:
lower income is consequential of lack of work and, thus, less access to
healthcare services. This situation also diminishes possibilities for
access to antiretroviral therapy and to integral healthcare services,
which contributes to worsening of psychological and physical conditions
of individuals affected by AIDS and their families. The results confirm
statements made by other authors in that the quality of life of
individuals with HIV/AIDS is a complex constellation of disease,
poverty, stigma, discrimination, and lack of treatment.
This
study did not reveal a statistically significant association between
quality of life and gender. A significant relationship was only
identified in one of the dimensions in the quality-of-life scale,
concerns about health and gender, showing that women have a lower
quality of life with respect to concerns generated by their health
condition. Relationships with the adherence variable are not presented
in this article.
CONCLUSION
Frequency of signs and
symptoms and taking ARV medications were the variables most associated
to quality of life in inverse relationship for the first, i.e., a
greater number of signs and symptoms indicate lower quality of life;
and in direct association, for the latter, meaning better quality of
life among those receiving medications. These aspects correlate with
the natural history of the disease, which has shown that the benefits
of antiretroviral therapy in terms of the prognosis are greater than
the adverse effects noted specifically at the beginning of therapy.
These findings agree with those reported by other authors like Wu12.
Improving the immune system and diminishing viremia translates to
lesser symptoms, lowered options of developing opportunistic
infections, and greater chances of reinsertion into the social
environment and the labor market. These factors are undoubtedly
reflected in the different dimensions measuring quality of life. Figure 2
presents the scheme of the variables related to global quality of life
and with their dimensions in individuals living with the AIDS virus.
Implications for practice and research. The
HIV/AIDS disease is a public health issue, given the dimensions of its
propagation. Given that it is a chronic disease, this study suggests
several challenges and questions to address from different disciplines,
especially from the field of nursing: How to improve in society and in
nursing care the quality of life of individuals living with the AIDS
virus?
·
Health professionals and society in general can adopt positive
attitudes and educate their patients to live better with HIV/AIDS.
· Healthcare
services must adequately and continuously provide medications to their
users so they can keep their illness under control.
· Nursing can teach and support strategies to reduce functional limitations such as nutrition and exercise.
· Nursing can
provide support and education for self-care and family care that
contribute to diminishing the frequency and intensity of the symptoms.
· Maintaining a
good quality of life requires healthcare with a holistic and integral
focus, given the different dimensions that define it.
Limitations.
This study was conducted on a non random sample of patients among those
attending health ambulatory medical and nursing control services in
three healthcare institutions in the city of Cali. The results can be
extrapolated to patients with similar characteristics, which is why we
recommend further studies with random samples of patients.
Conflict of interest. None of the authors has conflicts of interest related to this study.
ACKNOWLEDGMENTS
This study was funded
by the Colombian Institute for the Development of Science and
Technology (COLCIENCIAS) through contract Nº 11060416327 and by
the School of Nursing at Universidad del Valle in Cali, Colombia.
REFERENCES
1. Valencia CP, Canaval GE,
Rizo V, Correa D, Marín D. Signos y síntomas en personas
que viven con el virus del SIDA. Colomb Med. 2007; 38: 365-74.
2. Nicholas PK, Kemppainen
JK, Canaval GE, Corless IB, Sefcik EF, Nokes KM, et al. Symptom
management and self-care for peripheral neuropathy in HIV/AIDS. AIDS
Care. 2007; 19: 179-89.
3. Nicholas P, Voss J,
Corless I, Lindgren T, Wantland D, Kemppainen J, Canaval GE, et al.
Unhealthy behaviors for self-management of HIV-related peripheral
neuropathy. AIDS Care. 2007; 19: 1266-73.
4. Centers for Disease
Control and Prevention (CDC). Measuring healthy days. Population
assessment of health- related quality of life. Atlanta: CDC; 2000.
5. Ferrans CE. Quality of life: Conceptual issues. Semin Oncol Nurs. 1990; 6: 248-54.
6. Nokes MK, Coleman C,
Hamilton MJ, Corless IB, Selcik E, Kirsey K, et al. Health-related
quality of life in persons younger and older than 50, who are living
with HIV/AIDS. Res Aging. 2000; 22: 290-310.
7. Phaladze NA, Human S,
Dlamini SB, Hulela EB, Hadebe IM, Sukati NA, et al. Quality of life and
the concept of living well with HIV/AIDS in sub-Saharan Africa. J Nurs
Schol. 2005; 37: 120-6.
8. Palella FJJr, Delaney KM,
Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining
morbidity and mortality among patients with advanced human
immunodeficiency virus infection. HIV Outpatient Study Investigators.
New Engl J Med. 1998; 338: 853-60.
9. Holzemer WL, Henry SB,
Nokes KM, Corless IG, Brown M, Powell Cope GM, et al. Validation of the
sign & symptom check list for persons with HIV disease
(SSCHIV). J Adv Nurs. 1999; 3: 1041 49.
10. Holzemer WL, Hudson A,
Kirskey K, Hamilton MJ, Bakken S. The revised sign and symptom check
list for HIV (SSC-HIV rev). J Assoc Nurs AIDS Care. 2001, 12: 60 -70.
11. Holmes WC, Shea JA. A new
HIV/AIDS-targeted quality of life (HAT- QoL) instrument: development,
reliability, and validity. Med Care. 1998; 36: 138-54.
12. Wu AW, Dave NB,
Diener-West M, Sorensen S, Huang, IC, Revicki DA. Measuring validity of
self-reported symptoms among people with HIV. AIDS Care. 2004; 16:
876-81.
13. Lorenz KA, Shapiro MF,
Asch SM, Bozzette SA, Hays RD. Associations of symptoms and
health-related quality of life: findings from a national study of
persons with HIV infection. Ann Int Med. 2001; 134: 854-60.
14. Préau M, Leport C,
Salmon-Ceron D, Carrieri P, Portier H, Chene G, et al. Health-related
quality of life and patient-provider relationships in HIV-infected
patients during the first three years after starting PI-containing
antiretroviral treatment. AIDS Care. 2004; 16: 649-61.
15. Bing EG, Hays RD,
Jacobson LP, Chen B, Gange SJ, Kass NE, et al. Health-related quality
of life among people with HIV disease: Results from the multicenter
AIDS cohort study. Qual Life Res. 2000; 9: 55-63.
16. Call SA, Klapow JC,
Stewart KE, Westfall AO, Mallinger AP, DeMAsi RA, et al. Health-related
quality of life and virologic outcomes in an HIV clinic. Qual Life Res.
2000; 9: 977-85.
17. Hays RD, Cunningham WE,
Sherbourne, CD, Wilson IB, Wu AW, Cleary PD, et al. Health-related
quality of life in patients with human immunodeficiency virus infection
in the United States: results from the HIV cost and services
utilization study. Am J Med. 2000; 108: 714-22.
18. Sousa KH, Holzemer WL,
Henry SB, Slaugther R. Dimensions of health-related quality of life in
persons living with HIV disease. J Adv Nurs. 1999; 29: 178-87.
|