Effectiveness the pharmaceutical care in diabetic patients*
Jorge E. Machado-Alba, MD1, Sandra Torres-Rodríguez, Quim Farm2, Alvaro Vallejos-Narváez, MD3
* This research work was funded in part by Audifarma SA and Universidad Tecnológica de Pereira, Colombia.
1. Director Research Group on Pharmacoepidemiology and Pharmacosurveillance, Faculty of Health Sciences, Universidad Tecnológica de Pereira, Colombia. Specialized Professional, Department of Pharmacoepidemiology, Audifarma SA, Pereira, Colombia. e-mail: machado@utp.edu.co
2. National Coordinator of Pharmaceutical Care, Department of Pharmacoepidemiology, Audifarma SA, Pereira, Colombia. e-mail: satorrero@yahoo.es
3. Sudirector Department of Pharmacoepidemiology, Audifarma SA, Pereira, Colombia. e-mail: agvallejos@gmail.com
Received for publication May 21, 2009 Accepted for publication September 28, 2010
SUMMARY
Objective: To determine the effectiveness of pharmaceutical care to improve control of type-2 diabetes mellitus.
Methods: We carried out pharmacotherapeutical intervention during 19 months on patients with type-2 diabetes mellitus who were affiliate members of the contributive regime of the General System for Healthcare and Social Security in Bogotá and Cartagena. Through an interview and evaluation of medical records, we obtained information about antidiabetic medications used, doses, other medications, along with Hemoglobin A1c level, arterial pressure, serum low-density lipoprotein cholesterol level, nephropathy screening, retinal screening, foot exams in the last year and problems associated with medication use by means of the DADER method Negative Outcomes Associated with Medication (NOM).
Results: The study had a sample of 143 patients (64 intervened and 79 controls) with female predominance (67.1% and 53.1%, respectively), mean age of 63.9±11.2 years. The patients in both groups were taking an average of 6.0±2.7 medications. Initial HbA1c mean was 7.7% and 7.8%, without improvement by the end of the study (7.4% for those intervened and 7.8% for the control group). Hypertension (81.1%) and dyslipidemia (62.9%) were the most important comorbidities. About 50.4% of NOM were of effectiveness, follows 31.3% of necessity. The mean cost per patient in controls was 1.4 greater than for the intervened group.
Conclusions: Increased effectiveness of the antidiabetic therapy was not demonstrated in patients intervened with pharmacotherapeutical monitoring, but we did obtain a reduction in healthcare costs.
Keywords: Diabetes mellitus; Glucosylated hemoglobin A; Hypoglycemic agents; Pharmaceutical services; Colombia.
Colomb Med. 2011; 42: 72-80
Efectividad del seguimiento farmacoterapéutico en diabéticos tipo 2
RESUMEN
Objetivo: Determinar la efectividad del seguimiento farmacoterapéutico para mejorar el control de los pacientes diabéticos tipo 2.
Métodos: Se realizó intervención farmacoterapéutica durante 19 meses a pacientes con diabetes mellitus tipo 2, afiliados al régimen contributivo del Sistema General de Seguridad Social en Salud en Bogotá y Cartagena. Mediante entrevista y revisión de la historia clínica, se obtuvo información sobre medicamentos antidiabéticos utilizados, dosis, comedicación, resultados en último año de HbA1c, tensión arterial, perfil lipídico, albuminuria, examen oftalmológico, valoración de pies y los Resultados Negativos Asociados con la Medicación (RNM) y se siguió la metodología DADER.
Resultados: Participaron 143 pacientes, 64 intervenidos y 79 controles, con predominio de mujeres (67.1% y 53.1%, respectivamente), promedio de edad 63.9±11.2 años. Los pacientes de ambos grupos tomaban en promedio 6.0±2.7 medicamentos. La HbA1c inicial tuvo un promedio de 7.7% y 7.8% y al finalizar el estudio los valores fueron de 7.4% y 7.8%, respectivamente en cada grupo. El 50.4% de los RNM fueron de efectividad, seguido de 31.3% de necesidad. En la visita inicial y final la recomendación farmacéutica fue aceptada y el problema de salud resuelto en 72 casos (42.9% de RNM) y en 46 casos (38.3% de RNM), respectivamente. El cociente medio del costo por paciente en el grupo control fue 1.4 veces mayor que en el intervenido.
Discusión: No se demostró aumento en la efectividad de la terapia antidiabética en pacientes intervenidos con seguimiento farmacoterapéutico, pero se consiguió una reducción en costos de la atención sanitaria.
Palabras clave: Diabetes mellitus; Hemoglobina A glucosilada; Agentes hipoglucémicos; Servicios farmacéuticos; Colombia.
Colomb Med. 2011; 42: 72-80
Diabetes mellitus (DM) is an increasingly occurring disease, which generates important complications that affect the quality of life of patients; hence, its care generates high costs, given that it is a disease of utmost interest for public health. DM affects 130-million individuals around the world, 35-million are in America, and nearly 19-million are in Latin America and the Caribbean. It is calculated that by 2025 there will be 300-million diabetics in the world and 40-million of these will live in our continent1-3. Diabetic patients do not adequately adhere to pharmacological or nutritional treatment, or to the recommended physical activity, which are required to reach a suitable metabolic control, leading to the emergence of micro and macrovascular complications4. It has been estimated that 7% of the Colombian population over 30 years of age suffers from type-2 diabetes and 30% to 40% are unaware of their condition1,4,5. Healthcare costs for diabetic patients in Europe vary from 758€ annually in 1998, to 1476€ in 20026,7.
To reduce health complications and costs in healthcare systems, strategies have been sought to contribute to such aims and which directly involve the pharmacist through a pharmaceutical care program, developed by Hepler and Strand in 19908; its objective is the optimization of the clinical results of the drug therapy, improvement of patient quality of life, contribution to the rational use of medications, and detection, prevention, and solution to Negative Outcomes Associated with Medication (NOM)9,10.
Pharmacotherapeutic Monitoring (PTM) is defined as the professional practice in which the pharmacist assumes responsibility for the needs of the patient related to medications. It is a useful tool for contributing to the adequate use of medications and guaranteeing their safe, effective, and economic use. All this based on good communication and cooperation between the patient and health personnel9.
NOM, according to the Third Concensus of Granada, are «health related problems or unwanted changes in the patient's state of health attributable to the use (or lack of use) of medications. To measure NOM, we used a clinical variable (symptom, signal, clinical event, metabolic or physiologic measurement, death), which does not fulfill the therapeutic objectives established for the patient». NOM are classified into problems of necessity, effectiveness, and safety; necessity NOM include untreated health problems and the effects of unnecessary medications, effectiveness NOM include the quantified and non-quantified ineffectiveness, and safety NOM include quantified and non-quantified lack of safety9,10.
There is evidence in different countries around the world that the lack of NOM detection and solution may lead to additional costs in the healthcare system. A study conducted in Spain in 2002 found that three out of every four patients admitted to emergengy services were because of an NOM11,12. There is also evidence in that the results of pharmaceutical care may lead to reduced utilization of healthcare services and to a lower number of medications prescribed13.
In Colombia sufficient evaluations have not been conducted on the results of pharmaceutical care. In Medellín, a study carried out by Agudelo et al.14, evaluated the economic impact of pharmaceutical intervention in general ambulatory care, revealing a savings in medications of US$931.16 and a savings in laboratory tests of US$554 per patient per year.
Given that different studies have not been able to show the efficacy of pharmacotherapeutic monitoring to better control the disease and even reduce healthcare costs, we suggest the need for said intervention to aid in optimizing the benefits in healthcare services for patients with chronic treatments. A study was developed to permit determining the efficacy of pharmacotherapeutic monitoring and NOM identification to improve metabolic control by reducing glycated hemoglobin (HbA1c) in patients with type 2 diabetes mellitus in two Colombian cities when comparing the usual care. Additionally, we sought to determine the costs of caring for these patients during the study period.
MATERIALS AND METHODS
An intervention study was carried out during 19 months, between May 2006 and January 2008, to evaluate the effectiveness of pharmacotherapeutic monitoring to reduce HbA1c in patients with type 2 diabetes mellitus. The study had the participation of three pharmacist, two pharmacoepidemiologist physicians, and the support of last semester phamacist students from Universidad Nacional de Colombia in Bogotá and Universidad de Cartagena in Cartagena. The study was conveniently conducted in these cities because there was trained personnel for said purpose.
Population and sample. From a universe of 3635 patients with type-2 diabetes, distributed in Bogotá (2960 patients) and Cartagena (675 patients), we selected a a sample of 223 patients over 18 years of age (181 from Bogotá and 42 from Cartagena), who were receiving antidiabetic medication. All were affiliated to two Healthcare Promotion Companies (EPS for its acronynm in Spanish) in these cities. A possible 10% loss of the number of patients in each group was calculated.
The sample size was estimated as the comparison of two proportions. The parameters were type-1 error at 0.05 and type-2 error at 0.2, with expected effectiveness of 0.45 and relative risk of 1.5. Using the random number table method, we assigned the groups in random and stratified manner; 112 in the intervention group, who had pharmacotherapeutic monitoring for 18 months; and 111 in the control group, who were merely interviewed at the beginning and at the end of the study. Each of the patients had a replacement selected randomly and with the same characteristics.
The study evaluated the following variables:
Inclusion criteria. Patients with type-2 diabetes mellitus, affiliated to the contributive regime of two EPS, who had continuity in antidiabetic treatment in the three months prior, defined by attendance to medical control and request for dispensing of normoglycemiant medication; these patients were over 18 years of age and accepted to participate in the study.
Exclusion criteria. Patients changing EPS during the study; those whose physical or mental state did not permit communicating with the interviewer; and patients who did not remain in the city selected for the study during the time it took to develop such.
Field work. The protocol was subjected to approval by the Bioethics Committee of the Faculty of Health Sciences at Universidad Tecnológica de Pereira in Colombia, as well as by the Ethics Committess of the participating EPSs (committee minutes 30 March and 24 April 2006), in the category of «minimum-risk research», according to Resolution N° 008430 of 1993 from the Colombian Ministry of Health, which establishes scientific, technical, and administrative norms for health research. All the patients were affiliated to the General System of Health and Social Security (SGSSS for its name in Spanish) and have no problems obtaining the medications; all were registered in the institutional program for diabetes control and, thus, were receiving the care established by guidelines for caring for this type of pathology.
The patients selected were notified by phone for their participation in the study; they were then summoned to be furnished the detais of their participation and to sign an informed consent form once they accepted to participate in the study. Patients in the intervention group were subjected to glycated hemoglobin at the start, at six months and at the end of the study; additionally, an initial interview was conducted with the pharmacotherapeutic record format, according to the DADER methodology9. The status of the condition was elaborated (including diagnosis, each of the medications being taken, doses and dose intervals). During the study, the patients were visited on at least three instances, establishing the NOMs in each visit. Patients in the control group were subjected to HbA1c measurement at the beginning and end of the study; they also had an initial interview with the pharmacotherapeutical record format, according to the DADER methodology. The status of the condition was also elaborated for this group and a final visit was conducted; thereby, detecting the NOM.
After identifying NOM in each patient, the pharmacist suggested for the patients in the intervention group activities to solve the health problem associated to medication use, socializing said activities with the healthcare team through a written documment. Upon changes in medication, a new condition status was established, which also evaluated the acceptance or non-acceptance of the physician's pharmaceutical recommendations.
Phone calls and visits were also made every four months to inquire about hospitalizations, visits to the general physician, specialist, and emergency services. Physicians from EPSs were informed on the objectives and benefits of the pharmaceutical monitoring study and of the importance of their active participation in the program to offer complete patient care.
Sources of information. Pharmacotherapeutic records were the primary source of information and the secondary sources were the clinical histories, the status of the condition, records of medications dispensed by quantities and costs, along with the data base from the EPS services with the records of services rendered to their users, appointments with their treating physicians, authorizations for paraclinical exams requested by the physicians, among others.
Analysis of information. The SPSS 15.0 for Windows statistical package was used for data analysis. Parametric and non-parametric hypotheses tests were run for related samples, comparing the initial and final glycated hemoglobin within the same groups. Because the statistics for hypothesis tests were not significant, we opted for a bivariate analysis for the quantitative parameters via hazard ratios. Statistical significance was established at p<0.05. A descriptive analysis was performed of the cost variable for each of the EPSs and in each of the groups. Additionally, we conducted an analysis of the increasing cost-effectiveness ratios for each EPS.
RESULTS
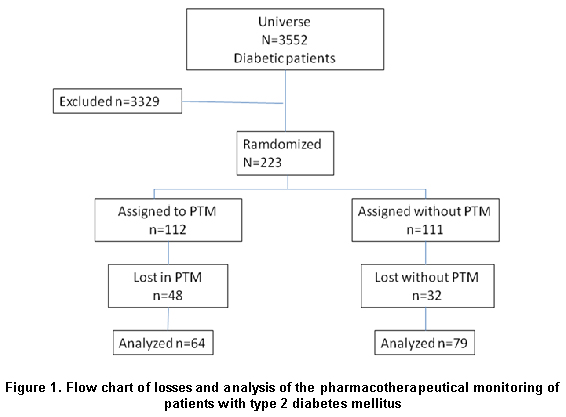
General findings. The study initially had 223 patients, 112 in the intervention group and 111 in the control group, but during the course of the study 80 patients were lost from the sample because of different causes, ending the study with 143 patients (64.1% of the original total) (Figure 1). Of the patients finishing the study, 143 were from Bogotá and 20 from Cartagena.
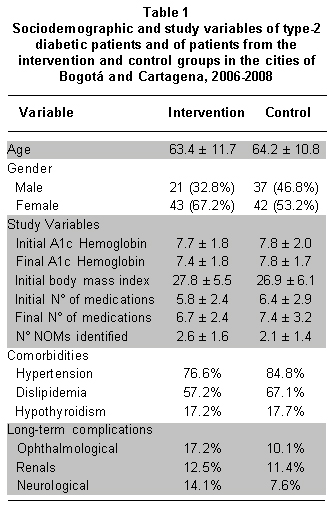
The distribution of the different study and sociodemographic variables can be seen in Table 1. Mean age was 63.9±11.2 years, ranging from 30 to 86 years of age. Upon comparing the initial average body mass index (BMI) with that of the final visit no statistically significant differences were found (p=0.09 and p=0.052, respectively); with a range between 18.5 and 40 kg/m2. Only 39 patients (27.3%) registered in the clinical history results of creatinine, eight patients (5.6%) revealed microalbuminuria, and only 25.9% of the patients registered a complete evaluation of the lipid profile and merely 7.7% were evaluated for thyroid stimulating hormone (TSH).
HbA1c findings and antidiabetic medication consumption. When comparing initial and final HbA1c values of the study, the average for the intervention group was 7.4% (p=0.0556; IC 95%: 7.0%-7.7%); and in the control group HbA1c was 7.8% (p=0.93; IC 95%: 7.3%-8.1%). Mean levels of initial basal glycemia were at 146 mg/dl for the intervention group and 143 mg/dl for the control group; while at the end of the study these values were 124 mg/dl vs. 136 mg/dl, respectively.
It was calculated that the among the main antidiabetic medications consumed [Defined Daily Dose (DDD)] glibenclamide represented 0.57 DDD per 1000 inhabitants/day, insulin 0.002 DDD per 1000 inhabitants/day, and metformin 4.61 DDD per 1000 inhabitants/day. It was found that on the average, the patients were receiving 1.17 of the DDD of glibenclamide, 1.61 of the DDD of insulin, and 0.86 of the DDD of metformin.
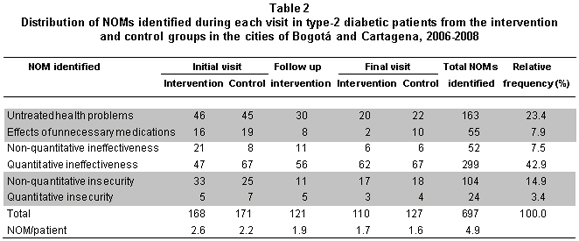
Co-morbidities and co-medication. The most prevalent co-morbidities were hypertension, dislipidemia, and hypothyroidism and the most frequent long-term complications can be seen in Table 2. We were able to identify in the patients in the study another 260 less prevalent health problems. We observed an average of 6.4±2.8 additional pathologies per patient for the intervention group and 6.0±2.4 for the control group, during the first visit. The most frequently identified co-medication corresponded to antihypertensive, hypolipidemic, thryroid hormone, antiplatelet drugs, among others.
Negative outcomes associated with medication. During each of the interviews of the patients in the intervention and control groups, we identified the NOM and the possible causes. Table 2 shows the NOM identified, with those relating to effectiveness being the most frequent (50.4%), followed by the necessity NOMs (31.3%). The greatest number of NOM was identified for antidiabetic medications with 232 cases (103 for metformin (44.4%), 72 for insulin (31%), and 57 for glibenclamide (24.7%); followed by 109 cases of antiplatelet drugs; then hypolipidemic drugs with 98 cases 78 for lovastatin (79.6%), 14 for gemfibrozil (20.4%), and 93 cases for antihypertensive medications.
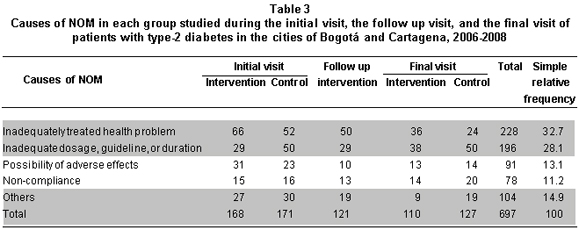
The most frequent NOM causes in these four pharmacological groups were thus: 126 (54.3%) of the NOMs associated to use of antidiabetic drugs were caused by inadequate dosage, guideline, or duration of the treatment; 98 (89.9%) of the NOMs associated to antiplatelet drugs were related to an insufficiently treated health problem; 40 of the hypolipidemic NOM (40.8%) were from the category belonging to insufficiently treated health problem; and 22 (23.6%) of the NOM associated to antihypertensive medications were caused by inadequate dosage, guideline, or duration of treatment. Causes of NOM identified in the study patients can be seen in Table 3.
Solution of negative outcomes associated with medication. During the initial and final visits for the intervention group, the intervention was accepted and the health problem was solved in 72 cases (42.9% of NOM) and 46 cases (38.3% of NOM), respectively. The intervention was accepted but the health problem was not solved in 21 cases (12.5%) during the initial visit and 16 cases (13.3%) during the final visit. The intervention was not accepted but the health problem was solved in 8 cases during the initial visit (4.8%) and 7 cases during the final visit (5.8%). The intervention was not accepted and the health problem was not solved during the first visit in 67 patients (39.9%) and during the final visit in 51 patients (42.5%). No important differences were found with the control group.
Costs. The descriptive analysis revealed the following: Total medical costs were $170'867,819 Colombian pesos (CP) for the 143 patients with whom the study was completed, distributed by $62'489,389 CP (36.6% of the cost) for the 63 participants from the intervention group and $108'378,430 CP (63.4% of the cost) for the 79 cases from the control group. The cost per thousand inhabitants per day (CID) was $228.7 CP for glibenclamide, $2,793.6 CP for insulin, and $3,256.3 CP for metformin.
Two cases were eliminated to diminish bias due to extreme values; the average direct cost per patient from the intervened group was $976,397 CP and $1'371,879 CP for the control group, during the study. It was noted that the mean ratio (average per patient) for the patients in the control group was 1.4 times greater than in the intervention group, suggesting that medical costs of patients from the intervention group were lower. Analysis per healthcare insurance carrier revealed that the difference in the mean ratio of the direct cost was in the range of 1.1 times to 2.5 times greater in patients from the control group, in relation to the intervention group; leading us to interpret that conducting pharmaceutical intervention is a more effective option in diminishing medical costs. It must be stated that the pharmacotherapeutic monitoring was carried out by the drug dispensing entity and not by the healthcare provider, for this reason the cost was not charged to the direct costs of patient healthcare.
DISCUSSION
Poor control of patients with type-2 diabetes mellitus is a problem affecting all nations. In developed nations as in developing nations, effectiveness of the therapy measured by controlling HbA1c figures ranges between 31.0% and 49.8%16-19. It is worth mentioning that in the study carried out, there was an important loss of patients (35.8%); hence, the authors are aware of the difficulties this generates in interpreting the results and the bias that can be generated, with the loss of patients being greater for the intervention group than in the control group (46.9% vs. 28.9%, respectively).
As with other studies, women were more willing to participate, which may be related to the greater prevalence of diabetes in this gender; with a mean age of 63 years and with overweight or obesity conditions16,20. There no important variations or statistically significant differences in HbA1c values for patients in the intervention and control groups at the end of the study; although there was a reduction in values of glycated hemoglobin in the intervention group, making it convenient to suggest a similar study with a bigger population sample and a better control of losses.
Along with other studies, during the initial interview, we found co-morbidities frequently associated to diabetes, such as hypertension (81.1%), dislipidemia (62.9%)16,20. Renal, ophthalmic, neurological, and vascular peripheral complications are very important in patients with type-2 diabetes, which contrasts with that found in the study, with scarce request for important tests like measurement of microalbuminuria, serum creatinine, lipid profile, and eye exam16.
The finding of a high percentage of ineffectiveness NOM (50.4%) is related to the poor control of type-2 diabetes mellitus in patients; although this disease needs multidisciplinary attention (adequate nutrition, regular physical exercise, healthy habits, and pharmacological treatment), monitoring with HbA1c is a good guide to make the pertinent adjustments to the treatment16.
The high frequency of the necessity NOM (31.3%) is probably associated to inadequate care of the patients, because of defficiencies in evaluating the disease, the co-morbidities, and the cardiovascular risk; particularly because of the underutilization of acetylsalicylic acid in secondary prevention in patients with high cardiovascular risk. Suggested interventions in pharmacotherapeutic monitoring, to correct this finding, may greatly benefit patients, possibly diminishing morbidity and mortality because of cardiocerebrovascular events associated to the use of said antiplatelet drug10.
Inadequate dossage (28.1%) was also identified as causing NOM, with daily defined dossages (DDD) lower than those established by the World Health Organization (WHO) for the different antidiabetic medications, especially for metformin. The adverse effects (13.1% identified for these medications) affect adherence and may aggravate patient morbidity.
The economic analysis between conducting interventions or keeping patients under habitual control, suggests to healthcare insurance carriers that implementing pharmacotherapeutic monitoring programs in patients with type-2 diabetes, may generate savings in costs related to caring for these patients. On the average, a patient from the intervention group generated a cost of $395,482 CP less than a patient from the control group during the 19-month study period. This finding warrants conducting a more profound study of the impact expected of pharmacotherapeutic monitoring on the cost of healthcare. Costs per 1000 inhabitants/day for each of the antidiabetic medications were lower than those reported by other studies carried out in Europe21.
This study presented a series of difficulties worth describing because they may be useful for those who may implement pharmacotherapeutic monitoring, such as: problems in obtaining a doctor's office for the interview between the pharmacist and the patients at the locations where the patients are normally cared. The need to schedule home visits requiring greater investment of time when the patient's health status does not permit attending the healthcare facility. Very frequently, the medical histories do not contain sufficient and necessary information for the case analysis in pharmacotherapeutical monitoring, given that many patients are seen by hired specialists, who generate reports different from those in the medical chart at the EPS, and access to this information is difficult in spite of multiple requests. Some treating physicians do not follow the guidelines for treatment of diabetes mellitus and do not make opportune requests for paraclinical and medical exams necessary for the complete analysis in pharmacotherapeutical monitoring. The researchers could not guarantee that the written reports with the intervention recommendations made by a pharmacist reached the treating physician; thus, the suggested intervention would or would not be accepted upon the detection of an NOM. Many of these difficulties came about because of the lack of support and commitment with the study from personnel in the participating healthcare insurance carriers.
The loss of 35.8% of the patients generated an important difficulty in analyzing the results to determine the effectiveness of pharmacotherapeutic monitoring of type-2 diabetic patients. The situations that could be related to the loss of patients include: prolonged duration of the study, change of EPS by several patients and change of address without notification of the new domicile, which made it difficult to locate the patient for the monitoring.
This study did not reveal increased effectiveness in treatment of patients with type-2 diabetes mellitus, which also occurred in the study by Beney et al.13; but a reduction was found in costs of medical care in the intervention group; along with determining the most important and most frequent NOM to suggest interventions destined to improving them.
In the future, in case pharmacotherapeutic monitoring is incorporated to daily care of diabetic patients, commitment is needed from healthcare insurance carriers (EPS) to make available the offices for the interviews, facilitate easier access to clinical records and paraclinical exams, updates of member addresses, generation of settings for meetings and discussion with treating physicians to socialize the NOM findings and the pharmaceutical recommendations, implement recommendations, and evaluate results. Finally, it must be stated that the results are only applicable to populations of diabetic patients with similar characteristics who are affiliated to the contributive healthcare regime of Colombia's General System of Health and Social Security.
Declaration of conflict of interest. The authors manifest and declare having no conflict of interest. One of the authors works for the two entities funding the study (Universidad Tecnológica de Pereira and Audifarma SA) and the other two authors work for Audifarma SA, without this affecting the contents of the manuscript.
ACKNOWLEDGEMENTS
We express gratitude to personnel from the Pharmacoepidemiology department at Audifarma SA, Paola Stefan, Tatiana Mendoza, Andrés Sáenz, Alfredo Portilla, and professor Jorge Augusto Díaz for their support in colecting and analyzing the information.
REFERENCES
1. Pan American Health Organization (PAHO). Diabetes in the Americas. Epidemiol Bull. 2001; 22:1-3.
2. European Molecular Biology Organization (EMBO). Like a snake in the grass. As the incidence of type 2 diabetes escalates, new developments offer hope for better treatments, reports. EMBO. 2004; 5: 555-8.
3. Asociación Latinoamericana de Diabetes. Guías ALAD de diagnóstico, control y tratamiento de la diabetes mellitus tipo 2. Rev Asoc Latinoam Diabetes. 2006; 14: 111-6.
4. Aschner P, King H, Triana de Torrado M, Rodríguez BM. Glucose intolerance in Colombia. A population-based survey in an urban community. Diabetes Care. 1993; 16: 90-3.
5. Aschner P. Diabetes trends in Latin America. Diabetes Metab Res Rev. 2002; 18: s27-31.
6. Oliva J, Lobo F, Molina B, Monereo S. Direct health care costs of diabetic patients in Spain. Diabetes Care. 2004; 27: 2616-21.
7. López BJ, Serrano AP, Duque GB. Los costes socioeconómicos de la diabetes mellitus. Aten Primaria. 2002; 29: 145-50.
8. Hepler C, Strand L. Opportunities and responsabilities in the Pharmaceutical Care. Am J Hosp Pharm. 1990; 47: 533-43.
9. Sabater D, Silva M, Faus M. Guía de seguimiento farmacoterapéutico: Método Dader, grupo de investigación en atención farmacéutica. 3a ed. Granada: Universidad de Granada; 2007.
10. Comité de Consenso. Tercer Consenso de Granada sobre problemas relacionados con los medicamentos y resultados negativos asociados a la medicación (RNM). (en línea). Ars Pharm 2007: 48: 5-17. URL disponible en: http://farmacia.ugr.es/ars/pdf/374.pdf.
11. Baena I. Problemas relacionados con los medicamentos como causa de consulta en el Servicio de Urgencias del Hospital Universitario Virgen de las Nieves de Granada. Tesis doctoral. Madrid: Ergo SA; 2004.
12. Silva M, Calleja M, Tuneo L, Fuentes B, Gutiérrrez M, Faus M. Seguimiento del tratamiento farmacológico en pacientes ingresados en un servicio de cirugía. Farm Hosp. 2004; 28: 154-69.
13. Beney J, Bero LA, Bond C. Expanding the roles of outpatient pharmacists: effects on health services utilisation, costs, and patient outcomes. Cochrane Database Syst Rev. 2000; CD000336. Review. Update in: Cochrane Database Syst Rev. 2010;7:CD000336.
14. Agudelo N, Cifuentes J, Amariles P. Impacto de la intervención del químico farmacéutico en el proceso de atención ambulatoria en una institución de salud en Medellín-Colombia. Pharm Care Esp. 2003; 5: 1-12.
15. Qaseem A, Vijan S, Snow V, Cross T, Weiss K, Owens D. Glycemic control and type 2 diabetes mellitus: the optimal hemoglobin A1c targets. A guidance statement from the American College of Physicians. Ann Intern Med. 2007; 147: 417-22.
16. Grant RW, Buse JB, Meigs JB, University HealthSystem Consortium (UHC) Diabetes Benchmarking Project Team. Quality of diabetes care in US academic medical centers: low rates of medical regimen change. Diabetes Care. 2005; 28: 337-442.
17. Liebl A, Mata M, Eschwège E, ODE-2 Advisory Board. Evaluation of risk factors for development of complications in Type II diabetes in Europe. Diabetologia. 2002; 45: S23-8.
18. Resnick HE, Foster GL, Bardsley J, Ratner RE. Achievement of American Diabetes Association clinical practice recommendations among US adults with diabetes, 1999-2002: The National Health and Nutrition Examination Survey. Diabetes Care. 2006; 29: 531-7.
19. Lebovitz HE. Oral antidiabetic agents: 2004. Med Clin North Am. 2004; 88: 847-63.
20. Machado-Alba JE, Moncada-Escobar JC, Gaviria H. Quality and effectiveness of diabetes care for a group of patients in Colombia. Rev Panam Salud Publica. 2009; 26: 529-35.
21. González P, Faure E, Del Castillo A, Grupo de Trabajo para el Estudio del Coste de la Diabetes. Cost of diabetes mellitus in Spain. Med Clin (Barc). 2006; 127: 776-84.