The association between population aging and oral and pharynx cancer incidence in the American continent
Michelle E. Denison, BSH, MPH1, Libia Soto, DDS2, Carlos A. Reyes-Ortiz, MD, PhD3
1. Research Assistant, Department of Social & Behavioral Sciences,
School of Public Health, University of North Texas Health Science
Center, Fort Worth, Texas. e-mail: mnail@live.unthsc.edu
2. Professor, School of Odontology, Universidad del Valle, Cali, Colombia. e-mail: libisotto@hotmail.com
3. Associate Professor, Department of Social & Behavioral Sciences,
School of Public Health, University of North Texas Health Science
Center, Fort Worth, Texas. e-mail: carlos.reyesortiz@unthsc.edu
Received for publication June 1, 2010 Accepted for publication December 21, 2010
SUMMARY
Objective: The objective of this study was to explore the association between aging of population and incidence of oral cavity and pharynx cancer at the country level in the American continent.
Methods: An ecological study at the country level. Countries' data for oral cavity and pharynx cancer incidence comes from the International Agency for Cancer Research (GLOBOCAN 2002). Twenty eight countries were included from North America, Central America, and South America. The dependent variables were the countries' oral cavity and pharynx cancer incidence rates (per 100,000/ year) by sex, overall and age-specific groups, 0-64 (younger population) and 65+ (older population), and the main independent variable was the countries' aging population (% of persons 65 years and older). Other variables considered were per-capita gross national income and prevalence of smoking by sex at the country level.
Results: Overall countries' level of oral cavity and pharynx cancer incidence rates were strongly correlated with the countries' aging population (p<0.01). In adjusted regression analyses, the countries' aging population was significantly associated with overall oral cavity and pharynx cancer incidence rates for male (p<0.0001, p=0.0003) and female (p=0.0025, p=0.0134) populations.
Conclusion: Countries' aging population was associated with increased countries' oral cavity and pharynx cancer incidence rates in the American continent.
Keywords: Oral cancer; Pharynx cancer; Aging; Population; Epidemiology.
Colomb Med. 2011; 42: 191-8
La asociación entre el envejecimiento de la población y la incidencia del cáncer oral y de faringe en el continente americano
RESUMEN
Objetivo: El objetivo de este estudio fue evaluar la asociación entre envejecimiento de la población y la incidencia de cáncer de la cavidad oral y de faringe en los países del continente americano.
Métodos: Estudio ecológico usando datos de cada país. Los datos por país para cáncer oral y faringe provienen de la Agencia Internacional de Investigación sobre el Cáncer (GLOBOCAN 2002). Veintiocho países de América del Norte, América Central y América del Sur, fueron incluidos. Las variables dependientes fueron las tasas de incidencia de cáncer de cavidad oral y de faringe (por 100.000/año) a nivel de cada país por sexo, en total y por grupos de edades 0-64 años y 65+ años, y la variable independiente principal fue el envejecimiento de la población a nivel del país (% de personas mayores de 65+ años). Otras variables consideradas fueron el ingreso nacional bruto per cápita y la prevalencia del fumar por sexo a nivel de cada país.
Resultados: Las tasas globales de incidencia del cáncer de la cavidad oral y de faringe de los países fueron correlacionadas significativamente con los porcentajes de envejecimiento poblacional de los países (p<0.01). En análisis de regresión linear ajustados, el envejecimiento poblacional de los países estuvo asociado significantemente con las tasas de incidencia globales del cáncer de la cavidad oral y de faringe para poblaciones masculinas (p<0.0001, p=0.0003) y femeninas (p=0.0025, p=0.0134).
Conclusión: El envejecimiento de la población a nivel de los países se asoció con mayores tasas de incidencia de cáncer de la cavidad oral y de faringe en el continente americano.
Palabras clave: Cáncer oral; Cáncer de faringe; Envejecimiento; Población; Epidemiología.
Colomb Med. 2011; 42: 191-8
Recent rising incidence rates of oropharyngeal squamous cell carcinoma, especially tonsilar and base-of-tongue cancer, may be caused by a new epidemic of sexually-transmitted human papillomavirus (HPV)1. In addition, there is an ongoing concern for the burden of oral cavity and pharynx cancer among developing countries, underserved populations, or minority ethnic groups2-4. For example, although the overall oral cavity and pharynx invasive cancer incidence and mortality rates have remained stable or even decreased among whites in the last decades, those rates have increased among blacks in the United States5. Also, in Brazil, living in deprived socioeconomic areas has been linked to higher mortality from oral and pharynx cancer6.
Risk factors reported in the literature for oral cavity and pharynx cancer include genetic predisposition, smoking, tobacco chewing, alcohol intake, mate intake, betel (areca nut), tooth loss and virus1,7,8. The 2005 International Agency for Research on Cancer evaluation on the carcinogenicity of HPV in humans concluded that there is sufficient evidence for the carcinogenicity of HPV-16 in the oral cavity and in the oropharynx, and limited evidence for HPV-18 in the oral cavity2,9. In contrast, fruits and green vegetables may protect against oral cavity and pharynx cancer10.
The mean age of the world's population is increasing because of a decline in fertility and a 20-year increase in the average life span during the second half of the 20th century11. These factors result in increased numbers of individuals aged >65 years during the next decades11. The America continent is also experiencing this demographic transition phenomenon11,12.
Cancer is a growing concern in the American continent13 and it is especially affecting the elderly14. Population aging has been associated with increased mortality for colorectal, bladder, stomach, and pancreas cancer15. However, the authors could not find reports in the literature linking population aging with oral cavity or pharynx cancer in the American continent. The objective of this study was to explore the association between population aging and incidence of oral cavity and pharynx cancer at the country level in the American continent.
METHODS
Design. A comparative ecological study examining an exposure-disease relationship between populations at one point in time was performed16; its unit of study was a country. Ecological studies were used to generate hypotheses in cancer epidemiology, but their results refer to populations of people and cannot be extrapolated to individuals17.
Data source. Cancer incidence rates come from the International Agency for Research on Cancer (IARC, from Lyon, France), GLOBOCAN 2002®, a statistical software package for cancer18. The IARC is a well-recognized institution that has had cancer statistics and publications for about 4 decades. This agency has incidence and mortality cancer data from the five continents. The methods to estimate the overall and sex age-specific incidence rates of cancer for a country fall into one of the following categories (GLOBOCAN 2002): 1. National incidence data: Puerto Rico, Costa Rica, Canada, and Cuba; 2. National mortality data or rates and proportions (e.g., from cancer registries) converted to incidence: Argentina, Brazil, Chile, Uruguay, the United States, Bahamas, Barbados, Belize, Bolivia, Guyana, Haiti, Nicaragua, Trinidad and Tobago, Venezuela, Paraguay, Peru, Suriname, Jamaica, El Salvador, Mexico, the Dominican Republic, Panama, Colombia, and Ecuador18. Data of the percentage of people 65 years of age and older for North American, Central American, Caribbean, and South American countries comes from the 2003 World Population Data Sheet19. Countries gross national income (GNI) data come from the 2003 World Population Data Sheet19, produced by the Population Reference Bureau and reporting data for the year 2001. Smoking prevalence (%) at the country level comes from the Tobacco Control Country Profiles 2003 from the American Cancer Society20. Because the study used no individual data but population data that is publicly available, application for approval from an ethics committee was not necessary.
Sample. From 30 countries with oral cavity and pharynx cancer data from GLOBOCAN 2002 for the American continent (North, Central and South America and the Caribbean), 2 countries (Honduras and Guatemala) were excluded because they had imputed data from neighboring countries18, leading to a sample of 28 countries.
Measures. The dependent variables were overall crude incidence rates and age-specific incidence rates for each cancer (oral and pharynx), and reported by male or female populations separately; rates are expressed per 100,000/year. The following cancers were included in the analyses: oral cavity (ICD-9 codes C00-C08) and pharynx (ICD-9 codes C09-C10, C12-C14)18.
The main independent variable was the countries' percentage of people 65 years of age and older, as a measure of aging of the population19,21. Other independent variables were GNI and prevalence of smoking in each country by gender. GNI per capita is gross national income in purchasing power parity (PPP) divided by the country's midyear population. GNI PPP refers to gross national income converted to «international» dollars by using the purchasing power parity conversion factor. International dollars indicate the amount of goods and services one could buy in the United States with a given amount of money19. GNI has been used in cross-country comparisons22. Smoking prevalence (%) at the country level is reported by sex (male and female adults)20.
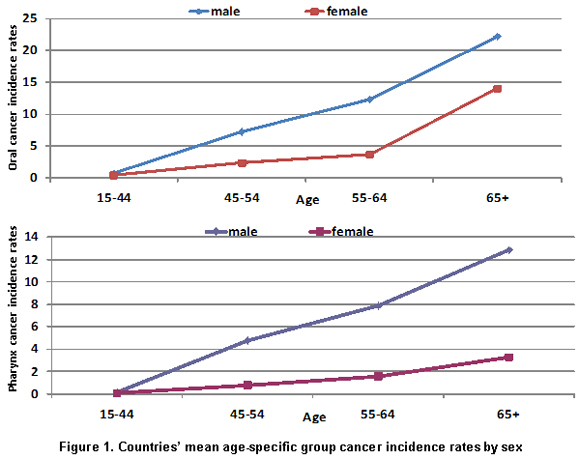
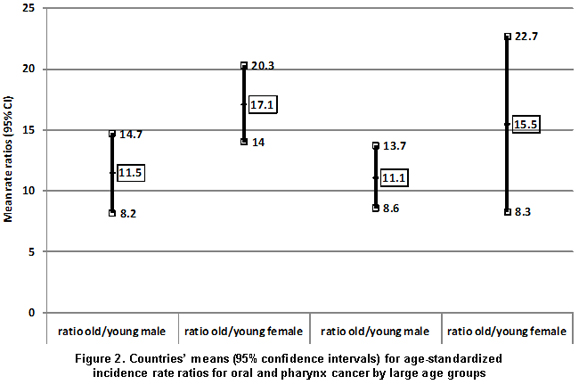
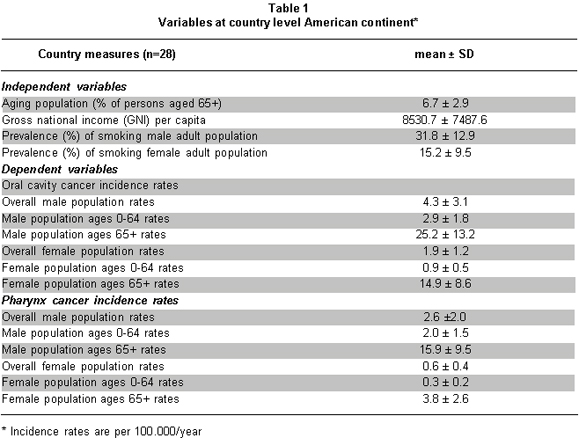
Statistical analysis. All statistical analyses were carried out using version 9.1 of SAS for Windows (SAS Institute: Cary, North Carolina). To describe the variables of the study at the country level, we used means (± SD) (Table 1). To describe the variation of age-specific cancer incidence rates by gender, we used graphics (Figure 1). To explore the difference on rates among large age groups (older vs. younger) and sex, we calculated cancer incidence rate ratios across those groups (Figure 2). To explore the association between population aging and incidence of oral cancer and pharynx cancer, we used Pearson (r) correlations analyses along with graphics (scatter plots with linear regression lines; Figure 3a, b) using the NCSS/PASS (Number Cruncher Statistical Systems: Kaysville, Utah) statistical software. One outlier (the Dominican Republic) that affected the regression line among data for women was removed from Figure 3b. Unadjusted linear regression analyses were performed for population aging predicting cancer incidence rates (Table 2). Adjusted linear regression analyses were performed for population aging predicting cancer incidence rates and controlling for the other variables. Since GNI had a skewed distribution, it was transformed to a natural logarithm for analyses. Regression models for pharynx cancer were adjusted for prevalence (%) of tobacco use at the country level but not for gross national income due to collinearity problems between GNI and population aging that were strongly correlated (r=0.69); collinearity is a potential problem seen in ecological analyses when variables are highly correlated among them16,17.
RESULTS
Table 1 shows the means (± SD) of the study variables used at the country level. Male populations had higher cancer incidence rates than female populations. Figure 1 shows the mean age-specific cancer incidence rates by sex in the American continent. Rates increased by age, especially at ages 55 and older. Males have the highest incidence rates for both oral cavity and pharynx cancer compared to female populations. Figure 2 shows the means (95% confidence intervals) of age-standardized incidence rate ratios for oral cavity and pharynx cancer per large age groups (younger= rates in ages 0-64; older= rates in ages 65+) in the American continent. Older male populations have about eleven times higher rates than younger male populations for both oral cavity (mean ratio=11.5) and pharynx cancer (mean ratio=11.1). That difference is larger for female populations (old/young mean ratios for oral cavity cancer=17.1, and for pharynx cancer=15.5).
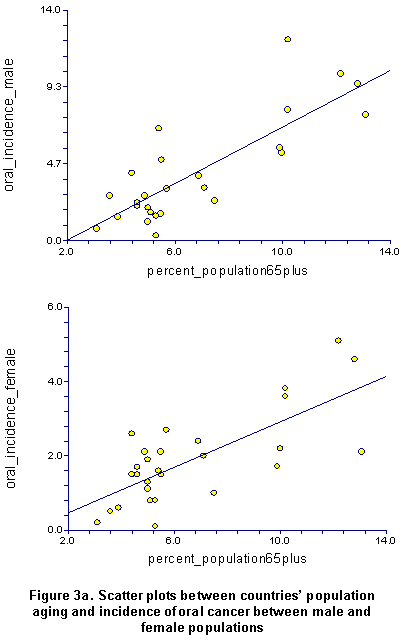
Figure 3a, shows the scatter plots with the linear regression lines between population aging and incidence of oral cancer among male and female populations in the American continent. Rates tend to increase as the percentage of population aging increases. There were strong and significant correlations between population aging and incidence of oral cavity cancer for both male (r=0.81, p<0.0001) and female (r=0.73, p<0.0001) populations.
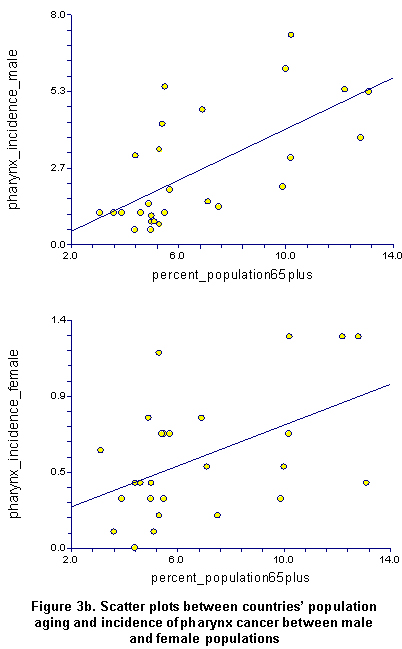
Figure 3b shows the scatter plots with the linear regression lines between population aging and incidence of pharynx cancer among male and female populations in the American continent. Rates tend to increase as the percentage of population aging increases. There were moderate and significant correlations between population aging and incidence of pharynx cancer for both male (r=0.56, p=0.0020) and female (without the outlier, as shown in Figure 3b, r=0.49, p=0.0091; with the outlier, data not shown, r=0.20, p>0.05) populations.
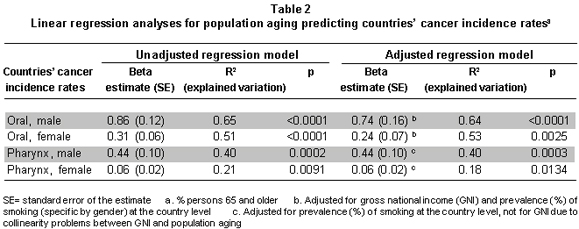
Table 2 shows that in adjusted regression analyses, population aging (percentage of persons 65 years and older) was a significant predictor for oral cavity and pharynx cancer incidence rates for male (p<0.0001, p=0.0003) and female (p=0.0025, p=0.0134) populations. Population aging explained between 21% and 65% of the variation (R2 values) in oral cavity and pharynx cancer incidence rates across countries. In additional unadjusted regression analyses, GNI was a significant predictor of oral cavity cancer incidence rates for male (p=0.0004) and female (p=0.0017) populations; similarly, GNI was a significant predictor of pharynx cancer incidence rates for both male (p<0.0001) and female populations (p=0.0051).
DISCUSSION
The objective of this study was to explore the association between countries' aging of population and incidence rates of oral cavity cancer and pharynx cancer in the American continent. We found that oral cavity cancer and pharynx cancer incidence rates were significantly associated with the aging of the countries' populations.
Population aging has been linked to increased cancer burden14,15. For example, the proportion of persons who are aged 65+ years with cancer include 81% for prostate, 74% colon, 72% pancreas, 70% urinary bladder, 68% stomach, 66% rectum, and 63% lung15. Population aging is one characteristic of the demographic transition phenomenon where there is a decrease in fertility rates along with low or moderate mortality rates and a greater number of individuals surviving 80 years and beyond21. Countries in demographic transition have evolved from predominantly rural to primarily urban societies. The association between population aging with oral cavity and pharynx cancer incidence in our study may reflect longer exposure time to environmental carcinogens and cumulative life-style changes (e.g., diet, sexual behaviors) in countries with complete or advanced demographic transition15,23. In other words, the cost for population longevity and economic progress could be an increase for oral cavity and pharynx cancer at the population level. Since most cancers appear at an advanced age, the burden of oral cavity and pharynx cancer could be heavier than that of other chronic diseases especially in populations with longer life expectancy.
Despite countries' oral cavity and pharynx cancer incidence rates for males being higher in our study than those for females, the difference in oral cavity cancer rates between older and younger populations is larger for females compared to males. These ecological findings generate a hypothesis to test in further studies at the individuals' level16,17, for example, to test whether older women have greater oral cavity cancer susceptibility than older men.
This study had some limitations. It was an ecological study, meaning that our findings may apply mostly to the country level but not to the individual level16,17,24. However, we used cancer data from the IARC that is a well-known source for cancer data around the world. Also, ecological studies are the basis for more complex study designs in cancer epidemiology16,17.
CONCLUSION
Oral cavity and pharynx cancer incidence rates among male and female populations were significantly associated with the aging of the population at country levels.
Conflict of interest. None of the authors has conflicts of interest related to this study.
REFERENCES
1. Attner P, Du J, Näsman A, Hammarstedt L, Ramqvist T, Lindholm J, et al. The role of human papillomavirus in the increased incidence of base of tongue cancer. Int J Cancer. 2010; 126: 2879-84.
2. Parkin DM, Almonte M, Bruni L, Clifford G, Curado MP, Piñeros M. Burden and trends of type-specific human papillomavirus infections and related diseases in the Latin America and Caribbean region. Vaccine. 2008; 26 (Suppl 11): L1-15.
3. Wunsch-Filho V. The epidemiology of oral and pharynx cancer in Brazil. Oral Oncol. 2002; 38: 737-46.
4. Polednak AP. Trends in incidence rates of tobacco-related cancer, selected areas, SEER Program, United States, 1992-2004. Prev Chronic Dis. 2009; 6: 1-12.
5. Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, et al. (eds). SEER Cancer Statistics Review, 1975-2006. National Cancer Institute. Bethesda. http://seer.cancer.gov/csr/1975_2006/, based on November 2008 SEER data submission, posted to the SEER web site, 2009.
6. Antunes JLF, Biazevic MGH, Araújo ME, Tomita NE, Chinellato LEM, Narvai PC. Trends and spatial distribution of oral cancer mortality in São Paulo, Brazil, 1980-1998. Oral Oncol. 2001; 37: 345-50.
7. Curado MP, Hashibe M. Recent changes in the epidemiology of head and neck cancer. Curr Opin Oncol. 2009; 21: 194-200.
8. Scully C, Bagan JV. Oral squamous cell carcinoma: overview of current understanding of aetiopathogenesis and clinical implications. Oral Dis. 2009; 15: 388-99.
9. IARC Monographs on the evaluation of carcinogenic risks to humans. Human Papillomaviruses. Vol. 90. Lyon: International Agency for Research on Cancer; 2007.
10. World Cancer Research Fund (WCRF)/American Institute for Cancer Research. Food, nutrition, physical activity for the prevention of cancer: a global perspective. Washington, DC: AICR; 2007.
11. Centers for Disease Control and Prevention (CDC). Trends in aging-United States and worldwide. MMWR Morb Mortal Wkly Rep. 2003; 52: 101-6.
12. Palloni A, Pinto-Aguirre G, Peláez M. Demographic and health conditions of ageing in Latin America and the Caribbean. Int J Epidemiol. 2002; 31: 762-71.
13. Bosetti C, Malvezzi M, Chatenoud L, Negri E, Levi F, La Vecchia C. Trends in cancer mortality in the Americas, 1970-2000. Ann Oncol. 2005; 16: 489-511.
14. Reyes-Ortiz CA, Camacho ME, Amador LF, Vélez LF, Ottenbacher K, Markides KS. Education, literacy and cancer screening among Latin American and Caribbean older adults. Cancer Control. 2007; 14: 388-95.
15. Yancik R. Cancer burden in the aged: An epidemiologic and demographic overview. Cancer. 1997; 80: 1273-83.
16. Borja-Aburto VH. Ecological studies. Salud Publica Mex. 2000; 42: 533-8.
17. Dos Santos Silva I. Cancer epidemiology: principles and methods. Lyon: International Agency for Research on Cancer; 1999.
18. Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2002: Cancer incidence, mortality and prevalence worldwide. IARC Cancer Base N° 5, version 2.0. Lyon: IARC Press; 2004.
19. Population Reference Bureau. 2003 World Population Data Sheet. Accessed at: http://demografia.rcm.upr.edu/World_Pob/World_Pop_2003.pdf.
20. Shafey O, Dolwick S, Guindon GE (eds). Tobacco Control Country Profiles 2003, Atlanta: American Cancer Society; 2003. Accessed at: http://www.wpro.who.int/internet/resources.ashx/TFI/TCCP2.pdf.
21. Brea J. Population dynamics in Latin America. Popul Bull. 2003; 58: 3-35.
22. Levin V, Tatsuzaki H. Radiotherapy services in countries in transition: gross national income per capita as a significant factor. Radiother Oncol. 2002; 63:147-50.
23. López-Ríos O, Lazcano-Ponce EC, Tovar-Guzmán V, Hernández-Ávila M. Breast cancer epidemy in Mexico: Demographic transition consecuence? Salud Pública Mex. 1997; 39: 259-65.
24. Diez-Roux AV. En defensa de la epidemiologia de números. Salud Colectiva. 2007; 3:117-9.