
Rectal damage control: when to do and not to do
Abstract
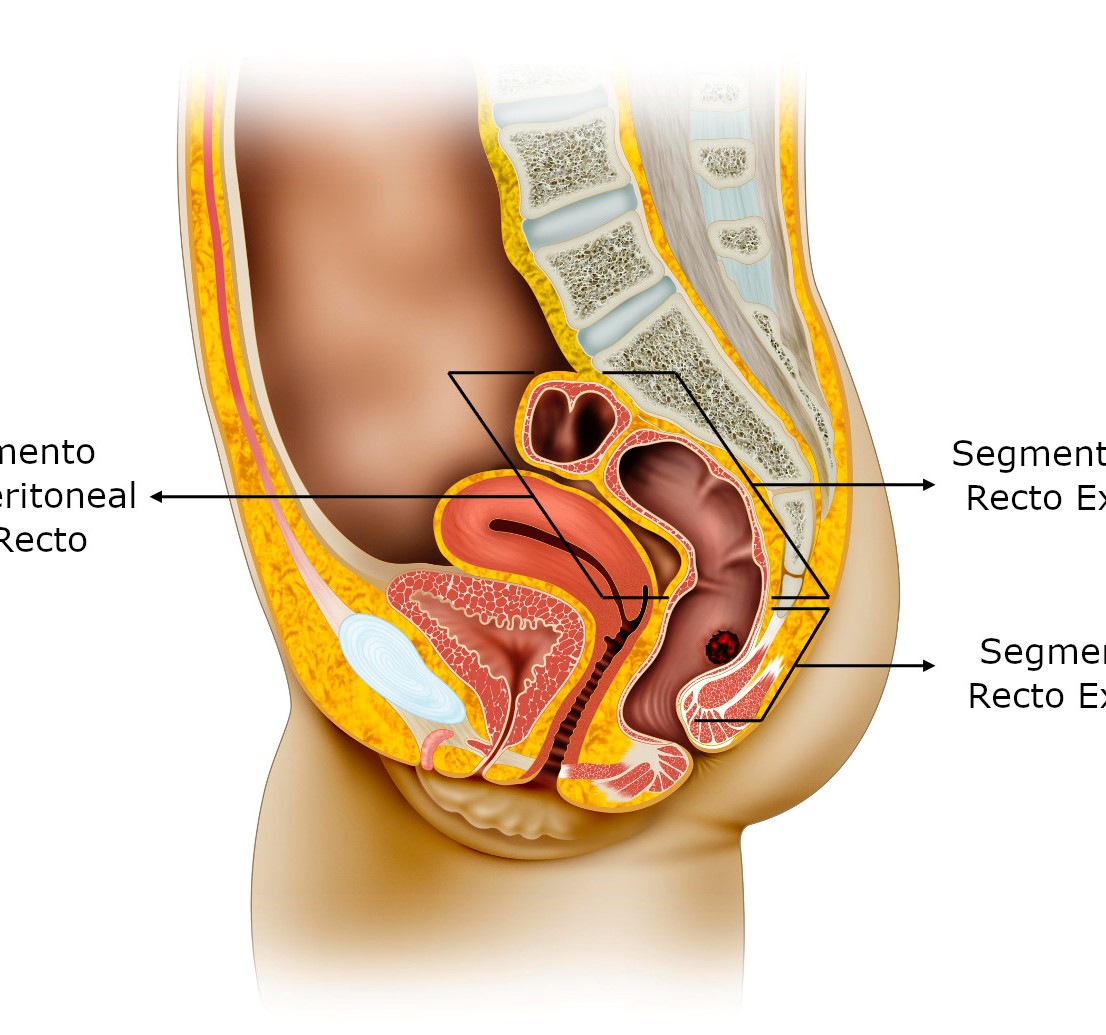
Rectal trauma is uncommon, but it is usually associated with injuries in adjacent pelvic or abdominal organs. Recent studies have changed the paradigm behind military rectal trauma management, showing better morbidity and mortality. However, damage control techniques in rectal trauma remain controversial. This article aims to present an algorithm for the treatment of rectal trauma in a patient with hemodynamic instability, according to damage control surgery principles. We propose to manage intraperitoneal rectal injuries in the same way as colon injuries. The treatment of extraperitoneal rectum injuries will depend on the percentage of the circumference involved. For injuries involving more than 25% of the circumference, a colostomy is indicated. While injuries involving less than 25% of the circumference can be managed through a conservative approach or primary repair. In rectal trauma, knowing when to do or not to do it makes the difference.
Authors
Downloads
Keywords
- Rectal Trauma
- Extraperitoneal Rectum Injuries
- Intraperitoneal
- Hemodynamically Unstable
- Hemodynamic Instability
- Damage Control
Author Biographies
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Hospital Universitario del Valle, Cali, Colombia.
 https://orcid.org/0000-0002-7955-8466
https://orcid.org/0000-0002-7955-8466
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia
https://orcid.org/0000-0002-6684-982X
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Hospital Universitario del Valle, Cali, Colombia.
https://orcid.org/0000-0002-1179-2854
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Hospital Universitario del Valle, Cali, Colombia. Centro Médico Imbanaco, Cali, Colombia
https://orcid.org/0000-0001-5862-4906
, Universidad Icesi, Cali, Colombia.
https://orcid.org/0000-0001-9081-5016
, Division of Colorectal Surgery, Department of Surgery, Fundacion Valle del Lili, Cali, Colombia
https://orcid.org/0000-0002-1577-5525
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia. Universidad Icesi, Cali, Colombia.
, Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia
https://orcid.org/0000-0002-5326-2317
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Centro Médico Imbanaco, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia. Universidad Icesi, Cali, Colombia
https://orcid.org/0000-0001-8187-0638
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Centro Médico Imbanaco, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia. Universidad Icesi, Cali, Colombia
https://orcid.org/0000-0001-9829-8930
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Hospital Universitario del Valle, Cali, Colombia.
, Department of Trauma Critical Care, Broward General Level I Trauma Center, Fort Lauderdale, FL – USA
https://orcid.org/0000-0001-6496-6275
, Division of Trauma and Acute Care Surgery, Department of Surgery. Universidad del Valle, Cali, Colombia. Division of Trauma and Acute Care Surgery, Department of Surgery. Fundación Valle del Lili. Cali, Colombia. Universidad Icesi, Cali, Colombia.
, Division of Colorectal Surgery, Department of Surgery, Fundacion Valle del Lili, Cali, Colombia
https://orcid.org/0000-0002-6163-4651
References
Steele SR, Maykel JA, Johnson EK. Traumatic injury of the colon and rectum: the evidence vs dogma. Dis Colon Rectum 2011; 54(09):1184-1201 https://doi.org/10.1007/DCR.0b013e3182188a60
Gonzalez RP, Phelan H III, Hassan M, Ellis CN, Rodning CB. Is fecal diversion necessary for nondestructive penetrating extraperitoneal rectal injuries? J Trauma 2006;61(04):815-819 https://doi.org/10.1097/01.ta.0000239497.96387.9d
Brown SR, Swisher JP, Hofmann LJ, Coviello LC, Davis KG. Surgical management and associated complications of penetrating rectal injuries sustained in Iraq and Afghanistan. Mil Med 2013; 178(11):1213-1217 https://doi.org/10.7205/MILMED-D-13-00167
Brown SR, Swisher JP, Hofmann LJ, Coviello LC, Davis KG. Surgical management and associated complications of penetrating rectal injuries sustained in Iraq and Afghanistan. Mil Med 2013; 178(11):1213-1217 https://doi.org/10.7205/MILMED-D-13-00167
Glasgow SC, Steele SR, Duncan JE, Rasmussen TE. Epidemiology of modern battlefield colorectal trauma: a review of 977 coalition casualties. J Trauma Acute Care Surg 2012;73(06, Suppl 5): S503-S508 https://doi.org/10.1097/TA.0b013e3182754759
Cho SD, Kiraly LN, Flaherty SF, Herzig DO, Lu KC, Schreiber MA. Management of colonic injuries in the combat theater. Dis Colon Rectum 2010;53(05):728-734 https://doi.org/10.1007/DCR.0b013e3181d326fd
Steele SR, Wolcott KE, Mullenix PS, et al. Colon and rectal injuries during Operation Iraqi Freedom: are there any changing trends in management or outcome?Dis Colon Rectum 2007;50(06):870-877 https://doi.org/10.1007/s10350-007-0235-4
Duncan JE, Corwin CH, Sweeney WB, et al. Management of colorectal injuries during operation Iraqi freedom: patterns of stoma usage. J Trauma 2008;64(04):1043-1047 https://doi.org/10.1097/TA.0b013e318047c064
Shannon FL, Moore EE, Moore FA, McCroskey BL. Value of distal colon washout in civilian rectal trauma-reducing gut bacterial translocation. J Trauma 1988;28(07):989-994 https://doi.org/10.1097/00005373-198807000-00013
DeBakey ME. Military surgery inWorldWar II; a backward glance and a forward look. N Engl J Med 1947;236(10):341-350 https://doi.org/10.1056/NEJM194703062361001
Stone HH, Fabian TC. Management of perforating colon trauma: randomization between primary closure and exteriorization. Ann Surg 1979;190(04):430-436 https://doi.org/10.1097/00000658-197910000-00002
Weinberg JA, Fabian TC, Magnotti LJ, et al. Penetrating rectal trauma: management by anatomic distinction improves outcome. J Trauma. 2006;60(3):508-514. https://doi.org/10.1097/01.ta.0000205808.46504.e9
Bosarge PL, Como JJ, Fox N, Falck-Ytter Y, Haut ER, Dorion HA, Patel NJ, Rushing A, Raff LA, McDonald AA, Robinson BR, McGwin G Jr, Gonzalez RP. Management of penetrating extraperitoneal rectal injuries: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2016. 80(3):546-51. https://doi.org/10.1097/TA.0000000000000953
Esposito TJ, Ingraham A, Luchette FA, et al. Reasons to omit digital rectal exam in trauma patients: no fingers, no rectum, no useful additional information. J Trauma 2005;59(06):1314-1319 https://doi.org/10.1097/01.ta.0000198375.83830.62
Hargraves MB, Magnotti LJ, Fischer PE, et al. Injury location dictates utility of digital rectal examination and rigid sigmoidoscopy in the evaluation of penetrating rectal trauma. Am Surg 2009;75(11):1069-1072 https://doi.org/10.1177/000313480907501108
Shlamovitz GZ, Mower WR, Bergman J, et al. Poor test characteristics for the digital rectal examination in trauma patients. Ann Emerg Med 2007;50(01):25-33, 33.e1 https://doi.org/10.1016/j.annemergmed.2007.01.022
Johnson EK, Judge T, Lundy J, Meyermann M. Diagnostic pelvic computed tomography in the rectal-injured combat casualty. Mil Med 2008;173(03):293-299 https://doi.org/10.7205/MILMED.173.3.293
Anderson SW, Soto JA. Anorectal trauma: the use of computed tomography scan in diagnosis. Semin Ultrasound CT MR 2008; 29(06):472-482 https://doi.org/10.1053/j.sult.2008.10.004
Schellenberg, Morgan et al. "The diagnostic yield of commonly used investigations in pelvic gunshot wounds." The journal of trauma and acute care surgery vol. 81,4 (2016): 692-8. https://doi.org/10.1097/TA.0000000000001159
Ordoñez CA, Parra M, Caicedo Y, Padilla N, Angamarca E, Serna J, Rodriguez F, Garcia A, Salcedo A, Pino L, Gonzalez Hadad A, Herrera M, Quintero L, Hernandez F, Franco M, Aristizabal G, Toro L, Guzman M, Coccolini F, Ferrada R, Ivatury R. Damage control surgical management of combined small and large bowel injuries in penetrating trauma: Are ostomies still pertinent? Colombia Medica. 2021;52(2):e4114425. https://doi.org/10.25100/cm.v52i2.4425
Ahern DP, Kelly ME, Courtney D, Rausa E, Winter DC. The management of penetrating rectal and anal trauma: A systematic review. Injury. 2017 Jun 1;48(6):1133-8 https://doi.org/10.1016/j.injury.2017.03.002
Atallah S, Albert M, De Beche-Adams T, Larach S. Transanal minimally invasive surgery (TAMIS): Applications beyond local excision. Tech Coloproctol . 2013. 17(2):239-43. https://doi.org/10.1007/s10151-012-0945-z
Copyright (c) 2021 Universidad del Valle

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
The copy rights of the articles published in Colombia Médica belong to the Universidad del Valle. The contents of the articles that appear in the Journal are exclusively the responsibility of the authors and do not necessarily reflect the opinions of the Editorial Committee of the Journal. It is allowed to reproduce the material published in Colombia Médica without prior authorization for non-commercial use




















